
Cialis ist bekannt für seine lange Wirkdauer von bis zu 36 Stunden. Dadurch unterscheidet es sich deutlich von Viagra. Viele Schweizer vergleichen daher Preise und schauen nach Angeboten unter dem Begriff cialis generika schweiz, da Generika erschwinglicher sind.
Gesundheitspsychologie.uni-mannheim.de
Journal of Abnormal Psychology
2012 American Psychological Association
2013, Vol. 122, No. 1, 45–50
Acute Exercise Attenuates Negative Affect Following Repeated Sad Mood
Inductions in Persons Who Have Recovered From Depression
Stanford University and University of Basel
Stanford University
Christian E. Waugh
University of Miami
Wake Forest University
Stanford University
Identifying factors that may protect individuals from developing Major Depressive Disorder (MDD) inthe face of stress is critical. In the current study we experimentally tested whether such a potentiallyprotective factor, engaging in acute exercise, reduces the adverse effects of repeated sad mood inductionsin individuals who have recovered from depression. We hypothesized that recovered depressed partic-ipants who engage in acute exercise report a smaller increase in negative affect (NA) and a smallerdecrease in positive affect (PA) when exposed to a repeated sad mood induction (i.e., habituation),whereas participants who do not exercise show sensitization (i.e., increased NA and decreased PA inresponse to a repeated adverse stimulus). Forty-one women recovered from MDD and 40 healthy controlwomen were randomly assigned to either exercise for 15 minutes or quiet rest. Afterward, participantswere exposed to two sad mood inductions and reported their levels of affect throughout the study.
Recovered depressed participants who had not exercised exhibited higher NA after the second sad moodinduction, a finding consistent with sensitization. In contrast, both recovered depressed participants whohad engaged in acute exercise and healthy control participants showed no increase in NA in response tothe repeated sad mood induction. Participants who exercised reported higher PA after the exercise bout;however, our hypothesis concerning reported PA trajectories following the sad mood inductions was notsupported. Results suggest that exercise can serve as a protective factor in the face of exposure torepeated emotional stressors, particularly concerning NA in individuals who have recovered fromdepression.
Keywords: exercise, recovered Major Depressive Disorder, sad mood induction, repeated stress, physicalactivity
Major Depressive Disorder (MDD) is one of the most prevalent
with vulnerability or protective factors (e.g.,
and burdensome of all psychiatric disorders. Importantly, MDD is
Vulnerability-stress formulations posit that the development of
a recurrent disorder; more than 80% of people with a history of
depression is due to the interaction of stressful events with one or
MDD have more than one episode of depression
more vulnerability factors. Similarly, protective models focus on
Investigators examining factors involved in the onset and
factors that may neutralize or reduce the impact of adverse expe-
recurrence of depression have focused on the interaction of stress
riences on the development of a negative outcome such as MDD
Depression is characterized by elevated levels of negative affect
(NA) and low levels of positive affect (PA), where NA represents
This article was published Online First September 17, 2012.
the extent to which individuals feel subjective distress and unplea-
Jutta Mata, Department of Psychology, Stanford University and Depart-
surable engagement, and PA the extent to which they feel enthu-
ment of Psychology, University of Basel; Candice L. Hogan and Ian H.
Gotlib, Department of Psychology, Stanford University; Jutta Joormann,
siastic, active, or alert Behav-
Department of Psychology, University of Miami; Christian E. Waugh,
iors that help to decrease NA and/or increase PA might act as
Department of Psychology, Wake Forest University.
protective factors in the face of stress. Acute exercise may be
This research was supported by Grant Wi3496/41 from Deutsche For-
one such factor. Engaging in acute exercise has been found to
schungsgemeinschaft to JM and NIMH Grant MH59259 to IHG. We thank
increase PA and result in fewer and less
Jessica Bowmer and Sarah Victor for their help with the study; Andrea
intense anxiety-related thoughts and attenuated physiological re-
Meyer and Rui Mata for advice on the article.
sponse following a psychosocial stressor
Correspondence concerning this article should be addressed to Jutta
Mata, Department of Psychology, University of Basel, Missionsstrasse
In a 1-week experience sampling
62a, 4055 Basel, Switzerland. E-mail:
study, found that depressed individuals had
MATA, HOGAN, JOORMANN, WAUGH, AND GOTLIB
higher levels of PA when they were physically active than during
Of these, four women were excluded because their scores on the
sedentary periods. Moreover, treatment studies with both unse-
Beck Depression Inventory-II (BDI-II;
lected and clinical samples have documented that engaging in
exceeded the cut-off (see requirements below), and two
prescribed exercise significantly reduces levels of depressive
dropped out before completing the second session, leaving a final
symptoms, including NA (e.g., Indeed, inves-
sample of 81 women. Forty-one had recovered from MDD based
tigators have found comparable benefits of treating MDD with
on the Structured Clinical Interview for DSM (SCID;
sertraline (an antidepressant medication) and with exercise after 4
and 40 were classified as
months and 6 months
never-disordered healthy control participants. Individuals were
Exercise can also reduce the likelihood of relapse of depression: in
excluded from participating in the study if they had experienced
10-month and 1-year
severe head trauma, learning disabilities, psychotic symptoms,
follow-up assessments, participants who exercised had signifi-
bipolar disorder, and/or alcohol or substance abuse within the last
cantly lower relapse rates than did participants who received
6 months. Women in the "recovered" group had to meet
DSM–IV
criteria for a past major depressive episode. To confirm full re-
Although most research concerning stress and depression has
covery from depression, participants completed a slightly modified
focused on the effects of major stressful life events like job loss or
version of the SCID using guidelines recommended by the NIMH
marital disruption, common repeated daily life adversities such as
Collaborative Program on the Psychobiology of Depression
family arguments or work deadlines also have a cumulative effect
Participants had to have eight consecutive
and impair health and well-being (e.g., Two
weeks with no more than two symptoms of no more than a mild
general learning processes that affect response to repeated adverse
degree (i.e., ratings of 1 ⫽
no symptoms or 2 ⫽
minimal symptoms,
experiences have been suggested: habituation and sensitization.
no impairment) in order to be classified as recovered from depres-
Habituation is defined as a decreased level of response to a
sion. Of the participants who had recovered from MDD, 11 par-
repeated stimulus; in contrast, sensitization refers to an increased
ticipants met criteria for a current Axis-I disorder, and 27 parti-
level of response to a repeated stimulus (e.g.,
cipants for a lifetime diagnosis of an Axis-I disorder. Healthy
For example, women have been found to
controls could not have had a past or current diagnosis of MDD or
exhibit higher heart rate and greater NA reactivity following a
any other Axis-I disorder and had to have a BDI-II score of 10 or
second than a first exposure to an adverse event, suggesting that
less. All participants were native English speakers and between 18
they became sensitized to the event
and 58 years old. Participants provided informed consent and were
compensated for their participation in the study. The Institutional
Investigators have not examined the effects of one bout of acute
Review Board at Stanford University approved the study.
exercise on the reaction to repeated stressors. In rodents, physicalactivity over time can facilitate habituation to repeated stressors:
compared with rodents that did not exercise, the cortisol response
Depressive symptoms were assessed
to an acute stressor in rodents that exercised decreased more
with the BDI-II, Cronbach's Alpha ⫽ .84.
rapidly as they were exposed to more stressors
Affect was assessed throughout the experimental ses-
Studying the effects of a 3-month
sion with the following two questions: "How positive are you
exercise training on response to a repeated stressor,
feeling right now?" and "How negative are you feeling right
randomly assigned 31 healthy men to an aerobic exer-
now?" on a 7-point Likert scale from 1 (
not at all) to 7 (
very) (cf.
cise program or a strength and flexibility program. Before and after
Before answering these scales for
the program, participants engaged in a stressful mental arithmetic
the first time, participants were thoroughly instructed on what was
task. Both groups showed a reduced physiological stress response,
meant by feeling positive and negative: At the far left of the PA
suggesting habituation; however, effects were stronger and applied
scale (1) they would feel completely neutral, neither positive nor
to a higher number of physiological markers in the aerobic exer-
negative; at the far right (7) they would feel very positive, such as
happy, pleased, satisfied, competent, or some other positive feel-
The present study was designed to examine experimentally the
ing. At the far right of the NA scale they would be feeling very
protective effect of exercise on affective responses to repeated
negative, which could be unhappy, frustrated, sad, depressed, or
stressors in individuals who have recovered from depression. We
some other negative feeling.
predicted that recovered depressed participants who engage in
Physical activity was assessed with the
acute exercise will report a smaller increase in NA and a smaller
7-Day Physical Activity Recall a
decrease in PA when exposed to repeated sad mood inductions
structured interview to determine minutes spent in physical activ-
(i.e., habituation), whereas recovered depressed participants who
ity over the course of an average week; results were converted into
do not exercise will show sensitization (i.e., increased NA and
weekly kilocalorie expenditure per kilogram of body weight.
decreased PA).
All participants viewed two film clips that
have reliably been shown to induce negative mood (see for a detailed description of the clips). Films were
Eighty-seven women were recruited through advertisements in
counterbalanced across participants and lasted approximately 6
local newspapers, Internet bulletin boards, and university kiosks.
minutes each.
AFFECT AFTER REPEATED STRESS AND ACUTE EXERCISE
Heart rate and respiration were re-
after the second sad film (i.e., approximately 8 minutes after the
corded with an integrated system and software package (Biopac
previous affect assessment). Participants were debriefed before
MP150, AcqKnowledge; Biopac Systems, Goleta, CA) at a sam-
leaving the laboratory.
pling rate of 1 kHz. Cardiovascular signals were recorded with theelectrocardiogram (ECG) amplifier module and pregelled dispos-
able electrodes. ECG data were scored offline using ANSLABsoftware inspected for artifacts, false
Demographic and Clinical Characteristics of
positives, and nonrecognized R-waves, and converted to heart rate(HR) using the corrected interbeat intervals. Exercise intensity
during cycling was determined using percent heart rate reserve
Participants who had recovered from MDD did not differ from
(HRR; HRR is operation-
healthy control participants in age, education, ethnicity, or physical
alized as the difference between resting and maximum heart rate.
activity level, but had significantly higher BDI-II scores than
HRR is preferable to the simpler age-predicted percent heart rate
healthy control participants (see
because it takes into account the possible range of an individual'sheart rate.
Manipulation Check 1: Effects of Exercise on Heart
Rate and Affect
Recovered and control participants did not differ significantly in
Participants meeting eligibility criteria in a telephone screen
baseline heart rate during rest (see Overall, participants
were invited to complete two separate sessions. In Session 1,
cycled at a mean of 34% HRR (see which constitutes
participants were administered the SCID. Our team of interviewers
mild exercise. Paired
t tests indicated that in the no-exercise
has previously achieved excellent interrater reliability for the as-
condition percent HRR was comparable in the baseline and resting
sessment of recovery from a major depressive episode (
k ⫽ .91)
periods,
t(36) ⫽ .22,
p ⫽ .83,
d ⫽ 0.04; in contrast, in the exercise
and for classifying participants as nonpsychiatric controls (
k ⫽ .92;
condition, percent HRR was significantly higher during the cycling
e.g., Next, the 7-Day Physical Activity
period than during baseline,
t(41) ⫽ 10.47,
p ⬍ .001,
d ⫽ 1.61.
Recall Interview was administered and participants completed
Participants in the exercise condition reported a significant
demographic and BDI-II questionnaires.
increase in PA between baseline and after the exercise bout,
Session 2 was conducted approximately 1 week later. Partici-
t(40) ⫽ ⫺3.53,
p ⫽ .002,
d ⫽ ⫺0.59, whereas participants in the
pants were asked to wear comfortable clothes in which they could
rest condition did not,
t(38) ⫽ 1.55,
p ⫽ .130,
d ⫽ 0.32. There was
move freely (e.g., t-shirt, sweat pants, sneakers) because we were
no change in NA between baseline and exercise bout in the
planning to measure their heart rate and breathing, possibly while
exercise condition,
t(40) ⫽ ⫺0.53,
p ⫽ .599,
d ⫽ ⫺0.14, or
they were moving, and it would be easier to attach sensors if they
between baseline and resting period in the rest condition,
t(38) ⫽
wore loose clothing. Furthermore, participants were asked to re-
0.27,
p ⫽ .786,
d ⫽ 0.04.
frain from participating in exercise on the day of the study and toconsume no more than their typical amount of caffeine 2 to 3 hours
Manipulation Check 2: Effect of Sad Mood Inductions
prior to their session. Of the 40 healthy control participants, 20were randomly assigned to an "exercise" condition and 20 to a "no
on Affect
exercise" condition. Of the 41 women recovered from MDD, 22
Paired
t tests showed that PA decreased,
t(79) ⫽ 10.05,
p ⬍
were randomly assigned to an "exercise" condition and 19 to a
.001,
d ⫽ 1.09, and NA increased,
t(79) ⫽ ⫺9.01,
p ⬍ .001,
d ⫽
"no-exercise" control condition.1 Physiological sensors were
1.46, after the first sad mood induction. After the second sad mood
placed on the participants, followed by a 5-min acclimation period.
induction, again, PA decreased,
t(79) ⫽ 10.60,
p ⬍ .001,
d ⫽ 2.04,
Next, participants rested quietly with eyes open while baseline
and NA increased,
t(79) ⫽ ⫺8.65,
p ⬍ .001,
d ⫽ ⫺1.56.
heart rate was recorded for 5 minutes. Participants assigned to theexercise condition cycled on a stationary bicycle for 15 minutes
Does Exercise Attenuate the Effect of Repeated Sad
(SensorMedics Ergometric 800 cycle ergometer, San Diego, CA)
at a speed and resistance they found comfortable. A meta-analysishas shown that most individuals choose mild to moderate activity
Means and standard deviations of the affect assessments are
as comfortable, which is the intensity level that leads to the
presented in Healthy control participants and participants
greatest improvement in affect Participants
recovered from MDD differed significantly in their levels of
assigned to the control condition were asked to rest quietly with
baseline negative affect,
F(1, 77) ⫽ 9.04,
p ⫽ .004, 2 ⫽ .15.
eyes open for 15 minutes. A selection of magazines was provided.
Despite the randomization, post hoc tests indicate a baseline dif-
Following completion of the exercise or control condition, partic-
ference in NA (
p ⫽ .024) between recovered MDD participants in
ipants sat quietly for 2 minutes. Participants then viewed a sad film
the exercise and control conditions; no baseline NA differences
and completed a 2-min information-processing filler task to givethem a short break. Next, they watched the second sad film. Affect
was assessed throughout the session: 10 minutes after arriving at
One participant did not complete the second affect assessment; her data
from this assessment are not included in the analyses. Physiological data
the laboratory, after the exercise/resting period (i.e., 17 minutes
from four participants (two recovered, two controls) could not be collected
after the previous affect assessment), after the first sad film (i.e.,
because of technical equipment malfunctions and were not included in the
approximately 6 minutes after the previous affect assessment), and
analyses of heart rate.
MATA, HOGAN, JOORMANN, WAUGH, AND GOTLIB
Table 1
Demographic Characteristics of Participants Recovered From MDD and Control Participants
Recovered from MDD; N ⫽ 41
Control; N ⫽ 40
Statistical difference values
Age;
M (
SD)
t(79) ⫽ ⫺0.11
Ethnicity (% Caucasian)
Education (% college graduates)
BDI-II score;
M (
SD)
t(79) ⫽ ⫺3.37*
Physical activity (kcal/kg; 7-Day PAR);
M (
SD)
t(77) ⫽ 1.22
Baseline heart rate
t(77) ⫽ ⫺1.18
% HRR cycling (Exercise group);
M (
SD)
t(40) ⫽ 1.67
% HRR rest (No exercise group);
M (
SD)
t(35) ⫽ 1.19
MDD ⫽ Major Depressive Disorder; BDI⫺II ⫽ Beck Depression Inventory⫺II; 7-Day PAR ⫽ 7-Day Physical Activity Recall Interview;
HRR ⫽ heart rate reserve.
*
p ⬍ .01.
were observed between control participants in exercise and rest
who have recovered from depression. As hypothesized, we found
conditions (
p ⫽ .583). Healthy control and recovered MDD par-
that both recovered depressed participants assigned to engage in
ticipants differed in baseline PA,
F(1, 77) ⫽ 4. 49,
p ⫽ .037;
acute exercise and healthy control participants (regardless of ex-
2 ⫽ .06; post hoc tests showed no differences in baseline PA
ercise condition) showed no increase in levels of NA in response
between the experimental conditions within either diagnostic
to a repeated stressor (i.e., sad mood inductions), whereas partic-
group (
ps ⬎ .2). Because of the differences between experimental
ipants recovered from MDD who did not exercise exhibited higher
conditions, we control for baseline NA in our analyses.
levels of NA after the second mood induction, suggesting sensiti-
To test whether the four groups of participants differed in levels
zation. However, in contrast to our hypothesis, we did not find any
of NA following the sad mood inductions, we conducted a 2
interaction between exercise condition and diagnostic group in
(diagnostic group; recovered, control) ⫻ 2 (experimental condi-
level of reported PA following the repeated sad mood inductions
tion; exercise, no exercise) ⫻ 3 (time: presad mood induction, after
that would be consistent with the notion of sensitization or habit-
first sad mood induction, after second sad mood induction) re-
peated measures analysis of covariance (ANCOVA) on NA ratings
The finding of higher NA after the repeated mood induction in
with baseline NA, BDI-II score, and physical activity as covari-
recovered depressed individuals who did not exercise is consistent
ates. This analysis yielded significant main effects of time,
F(2,142) ⫽ 3.51,
p ⫽ .033, 2 ⫽ .05, and an interaction of diagnostic
with results of previous studies. found a higher
group and time,
F(2, 142) ⫽ 4.78,
p ⫽ .010, 2 ⫽ .06. Although
risk of developing MDD for individuals with a short-allele in the
the omnibus three-way interaction was only marginally significant,
5-HTT genotype only if they had been exposed to repeated (two or
F(2, 142) ⫽ 2.00,
p ⫽ .105, 2 ⫽ .03, within-subject contrasts
more) stressful life events; there was no difference in the proba-
showed that the linear component of the three-way interaction of
bility of an adverse outcome if only one stressful life event had
diagnostic group, experimental condition, and time was signifi-
occurred. reported a similar pattern in rodents:
cant,
F(1, 71) ⫽ 4.71,
p ⫽ .033, 2 ⫽ .06 (the quadratic compo-
there was no difference in cortisol levels in response to an initial
nent of this interaction was not significant,
F(1, 71) ⫽ 0.06,
p ⫽
stressor between rodents that exercised and rodents that did not.
.810, 2 ⫽ .001).2 To explore the linear component of the three-
However, after being exposed to repeated stressors, rodents that
way interaction, we conducted planned contrasts, still controllingfor baseline NA, BDI-II score, and physical activity.3 Theseplanned contrasts indicated that this interaction was due to partic-
2 Whereas the control group was free of current psychopathology, 11
ipants who had recovered from MDD in the no-exercise group
participants recovered from depression met criteria for a different current
reporting higher levels of NA after the second mood induction than
psychopathology. Repeating our analyses excluding these participantsyielded comparable results: Again, the omnibus three-way interaction was
did participants in the three other groups,
t(76) ⫽ 2.97,
p ⫽ .004,
marginally significant,
F(2, 120) ⫽ 2.45,
p ⫽ .090, 2 ⫽ .04; the linear
d ⫽ 1.03 (see Importantly, planned contrasts for levels
component of the three-way interaction of diagnostic group, experimental
of NA presad mood induction and after the first sad mood induc-
condition, and time was significant,
F(1, 60) ⫽ 5.17,
p ⫽ .027, 2 ⫽ .08.
tion were not significant (
ps ⬎ .3). Also supporting our hypothesis,
We conducted planned contrasts despite
p ⬎ .05 for the overall
omnibus three-way interaction following
within the recovered depressed group, those who exercised re-
who argued that an omnibus-test only tests the null-hypothesis that
ported significantly lower levels of NA after the second sad mood
all groups in the analysis share a common population mean. If the omnibus
induction than did those who did not exercise,
t(39) ⫽ 2.65,
p ⫽
F-value is statistically significant, the null-hypothesis that all means are
.012,
d ⫽ 0.83. There were no significant main effects or interac-
equal is rejected. In our study, however, where three groups are expected
tions between exercise condition, diagnostic group, and reported
to be equal and one to be different, there is less power to detect thisdifference in an omnibus-test; indeed, there is a much higher probability
PA following the repeated sad mood inductions (all
ps ⬎ .1).
that an existing effect would be overlooked. Therefore, conducting a set ofcontrasts of conceptual interest, independent of the significance level of the
initial omnibus test, is recommended.
4 The mean % HRR is negative because participants' resting HR during
The present study was designed to assess experimentally the
acclimation was slightly higher than during the following resting period.
effects of exercise on responses to repeated stressors in individuals
This does not affect the interpretation of the results.
AFFECT AFTER REPEATED STRESS AND ACUTE EXERCISE
Table 2Affect Ratings
After exercise/rest
After 1st mood induction
After 2nd mood induction
M (SD)
M (SD)
M (SD)
M (SD)
Control, no exercise
Control, exercise
Recovered, no exercise
Recovered, exercise
Control, no exercise
Control, exercise
Recovered, no exercise
Recovered, exercise
exercised had a significantly lower cortisol response than rodents
difference between PA and NA (cf. Future
that did not.
research examining psychological and physiological mechanisms
Although participants in the exercise condition reported in-
that underlie the relation between exercise and response to re-
creased PA after the exercise bout as expected, our hypothesis
peated stressors might clarify such a difference in PA and NA
concerning reported PA following the sad mood inductions was
not supported. Power analyses suggest that the failure to support
This study has a number of theoretical and practical implica-
our hypothesis was not due to sample size. It is possible that the
tions. This is the first study to test experimentally the attenuating
experimental manipulation of sad mood inductions, which explic-
effects of exercise on levels of NA in the face of exposure to
itly targeted NA, led to a trajectory of PA that did not differentiate
repeated emotional stressors in individuals who have recovered
experimental conditions and diagnostic groups. This suggests that
from depression. Identifying such protective factors is an impor-
the interaction between exercise and response to repeated sad
tant contribution to research focused on understanding stress gen-
mood inductions works differently in PA and NA. Furthermore,
eration and stress sensitization in the context of the relation be-
the different findings for NA and PA support the conceptual
tween stress and depression. This is particularly important inindividuals recovered from depression who may be vulnerable toeven mild stressors In her review article onstress and depression, concludes that exposure torepeated or elevated rates of stressors likely predicts recurrence ofdepression, leading to a "self-perpetuating cycle of depression andstress" (p. 303). Thus, a better understanding of factors associatedwith reduced stress responding, such as mild exercise, would notonly contribute to a better understanding of vulnerability to recur-rent depression, but may also lead to the development of moreeffective interventions to prevent such recurrences. Our findingshighlight the effectiveness of low-intensity acute exercise to mit-igate the effects of stress resulting from sad-mood inductions inparticipants who have recovered from MDD. Despite recommen-dations of regular moderate-intensity aerobic exercise to maintaingeneral health the present finding is consis-tent with results of a recent meta-analysis indicating that mild-intensity acute aerobic exercise is optimal to improve positiveaffect This can have important implicationsfor adherence to an exercise regimen given that mild exercise, suchas light cycling or going for a walk, is easier to integrate intoeveryday activities than is moderate or intense planned exercise.
It is important to acknowledge three limitations of this study.
First, we assessed recovered depressed individuals in this study;future investigations should examine the effects of stress andexercise in participants with current MDD. Second, this is a
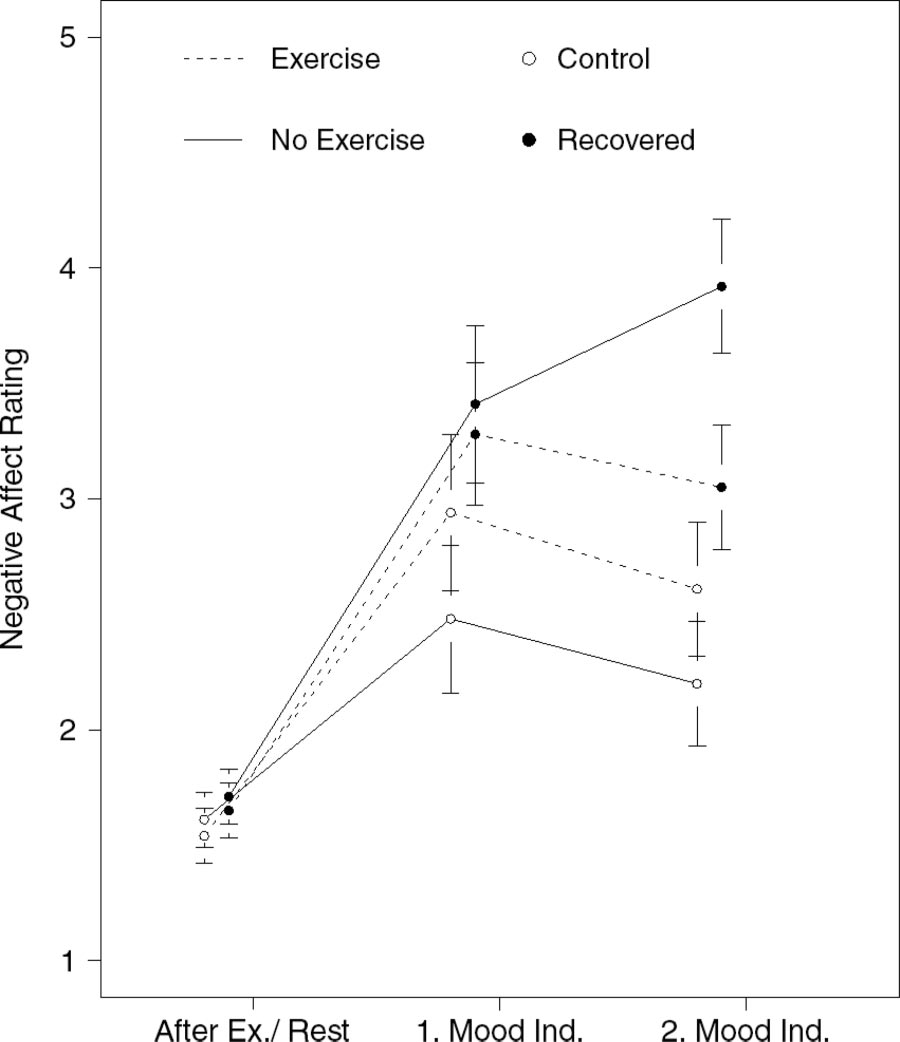
Negative affect ratings after exercise and sad mood inductions.
single-session laboratory experiment; therefore, the extent to
Error bars represent ⫾1 SEM. Negative affect ratings are estimated
which the findings generalize to multiple sessions over longer
marginal means, controlling for baseline negative affect, BDI-II score, andphysical activity. After Ex./Rest
periods of time, as well as to contexts outside the laboratory, must
⫽ After Exercise/Rest; Mood Ind. ⫽
Mood Induction.
be determined in future research. Third, because positive and
MATA, HOGAN, JOORMANN, WAUGH, AND GOTLIB
negative affect were measured with one item each, reliability
Joormann, J., & Gotlib, I. H. (2007). Selective attention to emotional faces
cannot be computed.
following recovery from depression. Journal of Abnormal Psychology,
It will be important in future research to systematically examine
116, 80 – 85.
psychological and physiological mechanisms that might underlie
Karvonen, M. J., Kentala, E., & Mustala, O. (1957). The effects of training
on the heart rate: A longitudinal study. Annales Medicinae Experimen-
the effects obtained in this study. Nevertheless, the present study is
talis et Biologiae Fenniae, 35, 307–315.
important in indicating that exercise— even at a comfortable, mild
Keller, M. B., Lavori, P. W., Mueller, T. I., Endicott, J., Coryell, W.,
level— can serve as a protective factor in the face of exposure to
Hirschfeld, R. M. A., & Shea, T. (1992). Time to recovery, chronicity,
repeated emotional stressors, particularly concerning NA in indi-
and levels of psychopathology in major depression: A 5-year prospective
viduals who have recovered from depression.
follow-up of 431 subjects. Archives of General Psychiatry, 49, 809 –816.
Kessler, R. C., & Wang, P. S. (2009). The epidemiology of depression. In
I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression (2nd ed.,
Almeida, D. M. (2005). Resilience and vulnerability to daily stressors
pp. 5–22). New York, NY: Guilford Press.
assessed via diary methods. Current Directions in Psychological Sci-
Levens, S. M., & Gotlib, I. H. (2010). Updating positive and negative
ence, 14, 64 – 68.
stimuli in working memory in depression. Journal of Experimental
Babyak, M., Blumenthal, J. A., Herman, S., Khatri, P., Doraiswamy, M.,
Psychology: General, 139, 654 – 664.
Moore, K., . . Krishnan, K. R. (2000). Exercise treatment for Major
Mata, J., Thompson, R. J., Jaeggi, S. M., Buschkuehl, M., Jonides, J., &
Depression: Maintenance of therapeutic benefit at 10 months. Psycho-
Gotlib, I. H. (2012). Walk on the bright side: Physical activity and affect
somatic Medicine, 62, 633– 638.
in Major Depressive Disorder. Journal of Abnormal Psychology, 121,
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck
Depression Inventory-II. San Antonio, TX: Psychological Corporation.
Mead, G. E., Morley, W., Campbell, P., Greig, C. A., McMurdo, M., &
Blumenthal, J. A., Emery, C. F., Walsh, M. A., Cox, D. R., Kuhn, C. M.,
Lawlor, D. A. (2009). Exercise for depression. Cochrane Database of
Williams, R. B., & Sanders Williams, R. (1988). Exercise training in
Systematic Reviews, 3.
healthy Type A middle-aged men: Effects on behavioral and cardiovas-
Nyhuis, T. J., Masini, C. V., Sasse, S. K., Day, H. E. W., & Campeau, S.
cular responses. Psychosomatic Medicine, 50, 418 – 433.
(2010). Physical activity but not environmental complexity, facilitates
Caspi, A., Sugden, K., Moffitt, T. E., Taylor, A., Craig, I. W., Harrington,
HPA axis response habituation to repeated audiogenic stress despite
H., . . Poulton, R. (2003). Influence of life stress on depression:
neurotrophin mRNA regulation in both conditions. Brain Research,
Moderation by a polymorphism in the 5-HTT gene. Science, 301, 386 –
1362, 68 –77.
Reed, J., & Ones, D. S. (2006). The effect of acute aerobic exercise on
Eisenstein, E. M., Eisenstein, D., & Smith, J. C. (2001). The evolutionary
positive activated affect: A meta-analysis. Psychology of Sport and
significance of habituation and sensitization across phylogeny: A behav-
Exercise, 7, 477–514.
ioral homeostasis model. Integrative Physiological & Behavioral Sci-
Rejeski, W. J., Thompson, A., Brubaker, P. H., & Miller, H. S. (1992).
ence, 36, 251–265.
Acute exercise: Buffering psychosocial stress responses in women.
Fergus, S., & Zimmermann, M. A. (2005). Adolescent resilience: A frame-
Health Psychology, 11, 355–362.
work for understanding healthy development in the face of risk. Annual
Sallis, J. F., Haskell, W. L., Wood, P. D., Fortmann, S. P., Rogers, T.,
Review of Public Health, 26, 399 – 419.
Blair, S. N., & Paffenbarger, R. S. J. (1985). Physical activity assessment
methodology in the Five-City Project. American Journal of Epidemiol-
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (2002). The
ogy, 121, 91–106.
Structured Clinical Interview for DSM-IV-TR Axis I disorders. New
Samanez-Larkin, G. R., Gibbs, S. E. B., Khanna, K., Nielsen, L.,
York, NY: New York State Psychiatric Institute, Biometrics Research.
Carstensen, L. L., & Knutson, B. (2007). Anticipation of monetary gain
Hammen, C. (2005). Stress and depression. Annual Review of Clinical
but not loss in healthy older adults. Nature Neuroscience, 10, 787–791.
Psychology, 1, 293–319.
Haskell, W. L., Lee, I. M., Pate, R. R., Powell, K. E., Blair, S. N., Franklin,
Schmaus, B. J., Laubmeier, K. K., Boquiren, V. M., Herzer, M., &
B. A., . . Bauman, A. (2007). Physical activity and public health:
Zakowski, S. G. (2008). Gender and stress: Differential psychophysio-
Updated recommendation for adults from the American College of
logical reactivity to stress reexposure in the laboratory. International
Sports Medicine and the American Heart Association. Medicine and
Journal of Psychophysiology, 69, 101–106.
Science in Sports and Exercise, 39, 1423–1434.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and vali-
Hoffman, B. M., Babyak, M. A., Craighead, W. E., Sherwood, A., Do-
dation of brief measures of positive and negative affect: The PANAS
raiswamy, P. M., Coons, M. J., & Blumenthal, J. A. (2011). Exercise and
Scales. Journal of Personality and Social Psychology, 54, 1063–1070.
pharmacotherapy in patients with Major Depression: One-year
follow-up of the SMILE Study. Psychosomatic Medicine, 73, 127–133.
Wilhelm, F. H., & Peyk, P. (2005). ANSLAB: Autonomic Nervous System
Laboratory (Version 4.0). Retrieved from
Jaccard, J., & Guilamo-Ramos, V. (2002). Analysis of variance frame-
works in clinical child and adolescent psychology: Issues and recom-
Received January 31, 2012
mendations. Journal of Clinical Child and Adolescent Psychology, 31,
Revision received July 18, 2012
Accepted July 24, 2012 䡲
Source: http://gesundheitspsychologie.uni-mannheim.de/Forschung/Publikationen/Mata%20et%20al.%20(2013).pdf
COMPOSANTES BIOLOGIQUES Quelques fondements de biologie moléculaire et de génie génétique intéressants pour approfondir le sujet, malgré le parti pris instructionniste qui sous-tend la présentation. Source : Centre Scientifique de la Biotechnologie/Industrie Canada http://strategis.ic.gc.ca/. Qu'est-ce qu'une cellule ? La cellule est l'unité du monde vivant et les millions de types différents d'organismes qui
Crenver Grove Management Plan 2006 The Sustainable Trust The Dandelion Trust This management plan was prepared by Tretec Ltd with input and advice from AJN Landscape Consultants MANAGEMENT PLAN OBJECTIVES SUMMARY OF MANAGEMENT PLAN SITE DESCRIPTION SITE DEFINITION AND BOUNDARIES WILDLIFE CONSERVATION VALUE DEVELOPMENTS & PAST MANAGEMENT ECOLOGY AND MANAGEMENT


