
Cialis ist bekannt für seine lange Wirkdauer von bis zu 36 Stunden. Dadurch unterscheidet es sich deutlich von Viagra. Viele Schweizer vergleichen daher Preise und schauen nach Angeboten unter dem Begriff cialis generika schweiz, da Generika erschwinglicher sind.
Rains.asn.au

Volume 4, Number 1 AUTUM N / WINTER EDITION 20 10
President's Report
SPECT/CT Bone Scan Skull
Overview of RAINS
Membership
What The ….?
Interesting Image
CPD Article
Crossword Puzzles
CPD Initiatives
INFORMATION
2010 Conference
2009 Report
Submission Guidelines
Membership Form
EMAIL CONTACT
New slett er: [email protected]
PO Box U102
M embership: [email protected]
Wagga W agga
Other: [email protected]
Seas RAINS, vol. 4, no. 1
President's Report
The Australian health care system has been
Welcome to the Autumn edition of Seasonal RAINS. I
described or defined by the „inverse care law‟; those
trust that the ANZSNM ASM in New Zealand will
Australians in the most need of health services
provide an opportunity for members and the RAINS
receive the least. This might equally reflect life for
Committee to exchange ideas. There are some
rural Nuclear Medicine professionals; those with the
important announcements in this edition so please read
greatest need for support and representation actually
have the least. It is true that the rural Nuclear
Medicine professional develops unique skills and
I would like to warmly welcome our new members,
capabilities not generally manifest in metropolitan
thank you for your interest and support. We now have
counterparts; an evolutionary adaptation („survival
155 associate members and 88 ordinary members. This
of the fittest‟). Despite these attributes, rural
Newsletter's success in previous years has been based
Nuclear Medicine professionals are confronted with
around the contributions of other members. I would
professional isolation that fosters a number of
like to encourage you all to send in those Interesting
Cases or Images we all stumble upon from time to
Professional representation at state and
time. It doesn't take much of an effort to email them
through for all of your colleagues to appreciate and
Accreditation and continuing professional
development (CPD).
Diffusion of innovation, technology and
The 2009 Annual CPD conference was held in October
last year at Diamond Beach near Forster. By all
Support for training, leave (illness or
accounts it was a huge success, with some great
recreation) and workload.
contributions from a broad spectrum of our regional
Career development pathways.
bases. It was located slightly off the beaten track, and
RAINS aims to quench the thirst of rural Australia
this assisted us with the decision to base this years
left parched by professional under representation.
conference in Sydney, providing all of our rural and
regional members more direct access.
RAINS Management Committee
The 2010 conference will be held at the Stamford
Mr Matt Ayers (NSW North) - president
Grand in North Ryde, adjacent to the new Macquarie
Mr Michael Crook (Qld South) – vice president
University Hospital. This year the theme is Integrative
Dr Geoff Currie (NSW South) - secretary
Imaging, and we are sure this will generate a great deal
Ms Narelle Harrison (Vic / Tas) - treasurer
of interest from all facets of Diagnostic Imaging, so
Mr Peter Tually (WA / SA)
don't miss out on the early bird deal. A brochure and
Mr Nathan Cassidy (QLD North / NT)
registration form has been included in this issue. Please
Mr Russell Pearce (associate member rep.)
encourage your CT, MRI and ultrasound colleagues to
Ms Annah Skillen (associate member rep.)
Easter is upon us already, this first quarter has literally
Dr Geoff Currie (editor-in-chief)
flown! For those of you fortunate enough to have an
Dr Janelle Wheat
affluent department, or generous boss, we may see you
Mr Michael Crook
in New Zealand for the Annual ANZSNM meeting. For
Mr Nathan Cassidy
the rest of us hard workers, the perfect opportunity to get the CPD points and catch up on the latest with your colleagues from around the country awaits in November with our RAINS conference.
See you all there!
Start Collecting
2010 is also an election year for RAINS. This means that members will be asked to nominate committee
members soon. Voting will then take place so that the new committee can take charge on 1 July 2010.
Matt Ayers
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Purpose of RAINS
Provide a network for support and collaboration
The purpose of RAINS is to offer a support network
Integrate student clinical placements
for rural and remote Nuclear Medicine
Lobby professional bodies on rural issues
professionals. The support network aims to engage
Promote Nuclear Medicine services in the rural
with and develop strategies to overcome the unique
professional difficulties encountered in rural and
Inform and lobby, where appropriate, legislative
remote Australia.
and regulatory processes impacting on rural
Nuclear Medicine
RAINS does not stand as an alternative to
ANZSNM state branch membership, but as an
Membership to RAINS is open to those Nuclear
Medicine professionals sharing the needs and
RAINS offers a seamless representation of rural and
philosophies characteristic of rural Australia;
remote Nuclear Medicine professionals. That is,
underpinned by "professional, social and cultural
RAINS is a single unified group of individuals with
isolation". To that end, membership is open to those
common needs and philosophy. There are neither
Nuclear Medicine professionals employed in a
state borders nor division between the private and
Nuclear Medicine practice that satisfies any one of
public sectors nor delineation based on corporate
the following criteria:
ownership. RAINS does respect and honour
1. Practice located in a centre that the Federal
commercial in-confidence and intellectual property
Government Rural, Regional and
Metropolitan Area (RRMA) classification
deems either rural or remote.
2. Practice located in a centre that is more than
Equitable provision of representation and
200 km from the state capital.
professional opportunities for rural and remote
3. Practice located in a centre that is more than
Nuclear Medicine professionals. Strategic
100 km from nearest other nuclear medicine
networking and support to foster professional
development, continuing education and
collaborative solutions to issues of isolation.
Associate membership to RAINS is open to:
Recognition and exploitation of distinctive
1. Students not actively employed in Nuclear
competencies of rural practitioners.
Medicine who are undertaking
undergraduate or post graduate studies in
Building A Future For Rural Nuclear Medicine
Nuclear Medicine at any Australian
university and who come from a RRMA
RAINS Core Values
classified rural or remote centre.
2. Nuclear Medicine professionals employed
Innovate, adapt, overcome.
in a Nuclear Medicine centre that does not
Be committed, meet our commitments.
meet the criteria for ordinary membership
Perform beyond industry norms.
but who believe issues of professional
Invest in our work, invest in ourselves.
isolation have a deleterious impact on
Improve, continually. Embrace innovation,
professional development. Examples of
embrace challenge.
such isolation include, but are not limited
Support CPD.
to; academics, researchers, company
Demand equity for rural Australia.
representatives and regional isolation with
Offer support, ask for support.
a small Nuclear Medicine network (e.g.
Exploit strengths, overcome weaknesses.
Newcastle, Central Coast, Gold Coast).
Membership entitlements include, but are not limited
Provide a voice and representation
Newsletter (electronic)
Overcome barriers to CPD
Networking (eg. research, problem solving,
Promote equity of service provision
reduce professional isolation)
Undertake research on rural issues
CPD activities (e-journal club, e-grand
Respect issues of commercial in-confidence
rounds, conferences)
BUT remove borders on core rural activities
Representation
Highlight and exploit the distinctive
competencies of the rural Nuclear Medicine
Full voting rights (ordinary members only)
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Interesting Image
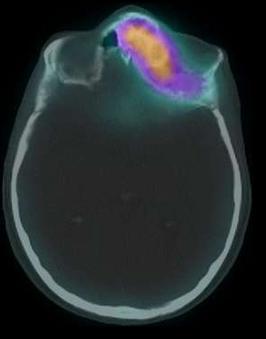
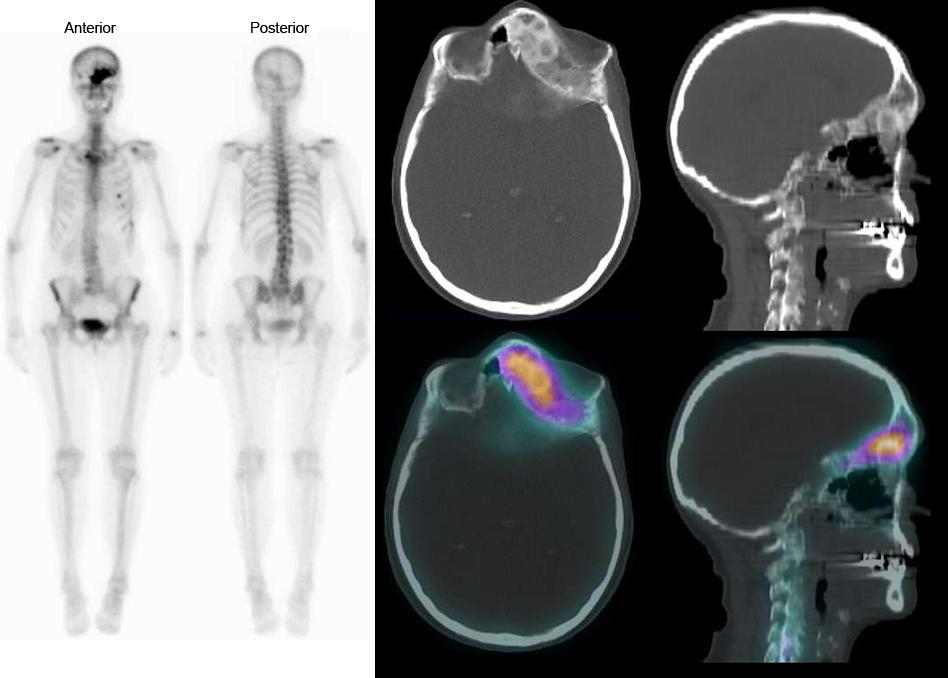
PRP Diagnostic Imaging, Sydney and Central Coast. Whole body bone scan on 72 yr old female with suspicious lesions in the cervical spine and possibly T4 on a recent MRI. No history of cancer. Incidental fall 1 week prior to scan.
Clinical
1. No evidence of skeletal metastatic disease. No
Fibrous dysplasia is monostotic in 70% of patients,
osteoblastic reaction in the cervical spine or T4.
with a predilection for long bones such as the femur,
2. Recent fracture involving the left trapezoid.
tibia, humerus, and rib. Most of these lesions are
3. Fibrous dysplasia in the inferior aspect of the left
found incidentally. Polyostotic fibrous dysplasia may
frontal bone (frontal sinus).
be extensive and frequently involves the femur
4. Subacute fractures in the 4th and 5th left ribs
(91%), tibia (81%), pelvis (78%), ribs, skull, facial
anterolaterally and 8th left rib laterally.
bones (50%), and less often the upper extremities,
lumbar spine, clavicle and cervical spine.
Overview
Fibrous dysplasia is a benign, intramedullary, fibro-
Monostotic fibrous dysplasia is craniofacial in 10%-
osseous lesion of bone that develops during skeletal
25% of patients but occurs in 50% with the
formation and growth and can be monostotic or
polyostotic disease. In the skull, the frontal,
polyostotic. Most often diagnosed in adolescents
sphenoid, maxillary, and ethmoidal bones are
and young adults, fibrous dysplasia accounts for
involved more often than the occipital and temporal
5%-7% of benign bone tumours. Most patients are
bones. Deformities include hypertelorism, cranial
asymptomatic and lesions are found incidentally,
asymmetry, facial deformity, visual impairment,
but patients can present with nonspecific swelling,
exophthalmos, and blindness due to orbital and peri
deformity or pain. Fibrous dysplasia is also
orbital bone lesions. Sphenoid wing and temporal
associated with several endocrine and non-
bone lesions may result in vestibular dysfunction,
endocrine disorders.
tinnitus and hearing loss.
The risk of malignant transformation is low (0.4%-
4.0%), but is more common in the polyostotic form.
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
disease in complex anatomic locations such as the
facial bones, pelvis, and spine. Attenuation of the
The typical radiographic appearance of fibrous
characteristic ground-glass portions is 70-130
dysplasia consists of a medullary-based, minimally
Hounsfield units (HU), in contrast to normal
expansile lesion with "ground-glass" opacity and
trabecular bone that is >250 HU. Lesions may
irregular but well-defined borders. In long bones,
expand bone. The mixed density of these lesions has
the location usually is diaphyseal or
been described as "whorls and swirls." Computed
diametaphyseal, and the epicentre is centric or
tomography can show compromise of the spinal
eccentric. More expansile lesions cause endosteal
canal and evaluate neural foraminal compromise in
scalloping and thinning that weakens the cortex.
the skull. In addition, signs of malignant
Lesional radiopacity is variable depending on the
transformation, including extraosseous soft-tissue
ratio of fibrous and osseous tissue. Homogeneous,
mass and aggressive bone destruction, can be shown.
featureless grey opacity is the classic "ground-
glass" appearance of fibrous dysplasia, a term
Bone Scan
borrowed from the appearance of frosted or ground
Fibrous dysplasia in general appears as an area of
window glass that is uniformly opaque. Lesions are
markedly increased uptake on bone scintigraphy,
less commonly homogeneously lucent or sclerotic.
however uptake may be normal or decreased. Barely
Chronic changes secondary to bone weakness may
increased bone uptake in fibrous dysplasia may be
lead to bowing of weight-bearing structures,
associated with decreased vascularity and
fracture, and remodelling.
osteoblastic activity of the lesion as a result of
concurrent bone infarction. Bone scans are not
Computed Tomography
helpful in diagnosing these lesions but can be useful
Computed tomography is not required for diagnosis
in identifying asymptomatic lesions.
but can be valuable in evaluating the extent of
Do you have an interesting image to share? Email the image and brief overview
with author details to [email protected]
Do you have a book review in mind or in progress? Email the final draft with
author details to [email protected] and collect 2 CPD points.
Do you have a journal article review in mind or in progress? Email the final draft
with author details to [email protected] and collect 2 CPD points.
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Continuing Professional Development
Brown Adipose Tissue and 18F-FDG PET.
Nuclear Medicine and PET, Hunter New England Imaging, Newcastle.
INTRODUCTION
muscular tension (Nedergaard, Bengtsson, &
The use of Fluorine-18 fluoro-2-deoxy-D-glucose
Cannon, 2007). The presence of BAT in these areas
(18F-FDG) in Positron Emission Tomography (PET)
has recently been confirmed histologically by
is now considered to be routine practice in oncology
Virtanen, et al. (2009) (Virtanen, et al., 2009).
as a tool for diagnosis, staging and assessment of
treatment response. 18F-FDG is used to assess the
BAT has been proven to exist in rodents throughout
function of active tumour cells through their
life and in human infants and young children
uncontrolled glucose metabolism (Evans, Tulloss, &
(Cypess, et al., 2009). However, it was a long held
Hall, 2007). Whilst 18F-FDG PET has a high
belief that in adult humans BAT was relatively non-
sensitivity for this purpose but specificity can be
existent with no physiological significance (Cypess,
problematic due to accumulation within several
et al., 2009). As a direct consequence of the
normal cells that also metabolise glucose, along
emergence of PET/CT technology, this belief was
with inflammatory and infective processes (Evans,
determined to be no-longer valid. In fact, Cohade, et
et al., 2007). The appearance of the brain and
al. (2003) documented the appearance of BAT on
myocardial cells on 18F-FDG PET is accepted, as a
PET/CT confirming its presence within adult
result of their glucose energy demands. Also not
humans, coinciding with the findings of other studies
uncommon is the visualisation of skeletal muscle,
(Cypess, et al., 2009; van Marken Lichtenbelt, et al.,
gastrointestinal tract, genitourinary tract, bone
2009; Virtanen, et al., 2009). Five common areas of
marrow, and lymphoid tissue for the same reasons
BAT have been identified (Nedergaard, et al., 2007)
(Evans, et al., 2007). Nuclear Physicians have also
to be within the neck and supraclavicular areas (more
noted areas of 18F-FDG accumulation within the
common) and the mediastinal (para-aortic),
supraclavicular and mediastinal areas that is not
paravertebral, and suprarenal areas (less common)
identified to corresponded to any areas of abnormal
(Nedergaard, et al., 2007). Hypermetabolic BAT
tissue on correlative imaging (Yeung, Grewal,
within these areas can affect the overall accuracy of
Gonen, Schoder, & Larson, 2003). This specific
18F-FDG PET in the investigation of lymphoma,
pattern was initially described to correspond to
oesophageal, stomach and lung cancers and also
muscular uptake in anxious patients, as the
metastatic lymph node involvement within the neck
administration of oral diazepam; a muscle relaxant,
and mediastinum (Cohade, Osman, et al., 2003).
and a repeat PET scan resulted in the reduction of
this uptake (Yeung, et al., 2003). Although
Hypermetabolic BAT is manageable and there is
considered normal variants, 18F-FDG uptake in
potential to eliminate the appearance on PET
these areas described can cause false-positive
imaging, but the nature and appearance BAT must be
findings (Williams & Kolodny, 2008) on PET
well understood.
Non-Shivering Thermogenesis
The introduction of PET/CT (Computed
Two types of adipose tissue exist; white adipose
Tomography) has allowed the fusion of PET and CT
tissue and brown adipose tissue (BAT), with two
images, allowing superior accuracy in the
types differing on a cellular level and also in their
localisation of abnormalities found on PET imaging
functionality (Cypess, et al., 2009). The primary
– a technique that cannot be achieved with such
purpose of white adipose tissue is the storage of
accuracy when PET and CT scans are undertaken
energy, whilst also providing insulation and
individually (Yeung, et al., 2003). Since PET/CTs
cushioning (Cypess, et al., 2009). On the other hand,
advent in 2001, several studies have been
the primary function of BAT is to provide warmth
undertaken to accurately localise the increased 18F-
through non-shivering thermogenesis (Cypess, et al.,
FDG accumulation within the supraclavicular and
2009). Microscopically, BAT is uniquely
mediastinal areas described above (Cohade, Osman,
characterised by abundant mitochondria and high
Pannu, & Wahl, 2003; Paidisetty & Blodgett, 2009;
vascularisation (giving the tissue its brown
Yeung, et al., 2003). This accumulation has been
appearance), and the presence of uncoupling protein
reported to correspond to areas of adipose tissue,
1 (UCP1) (Agrawal, Nair, & Baghel, 2009).
specifically hypermetabolic brown adipose tissue
Non-shivering thermogenesis is the process by
(BAT); as opposed to the previous conclusions that
which newborn infants and hibernating mammals
the accumulation is the result of anxiety induced
maintain normal body temperature through the
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
production of heat (Virtanen, et al., 2009; Weber,
The patterns of 18F-FDG uptake in BAT have been
2004). The identification of BAT on PET has
further defined (Yeung, et al., 2003) through an
proven that adults also have the potential to
analysis of 863 PET/CT examinations. This
maintain their body temperature through this
investigation determined four distinct areas of uptake
related to BAT, which was also described during
other investigations (Nedergaard, et al., 2007). 32
Adenosine triphosphate (ATP) is used an energy
patients were found to have hypermetabolic BAT
transporter between cells (Weber, 2004). In cells
(3.7%), which is a similar proportion of patients
other BAT, a proton gradient is observed across the
compared to previous investigations (Yeung, et al.,
mitochondrial membrane within the cell (Weber,
2003). Of significance is that 26 of these patients
2004). Energy derived from the flow of protons
were paediatric, which can be expected given that it
across this membrane allows adenosine diphosphate
is known that BAT is present within the younger
(ADP) to undergo oxidative phosphorylation and
population (Cypess, et al., 2009). This investigation
form ATP (Weber, 2004). In BAT cells, the
demonstrated a tendency towards female patients
presence of UCP1 allows protons to move along the
demonstrating higher BAT accumulation than males
protein gradient without causing ATP synthesis
(P<0.01) and no significant relation was found
(Weber, 2004). This process uncouples oxidative
between BMI and the appearance of BAT. Standard
phosphorylation and energy is converted to heat,
Uptake Value‟s (SUV) were calculated in patients
rather than being used for ATP synthesis (Celi,
demonstrating neck accumulation that was localised
2009; Weber, 2004).
to BAT (SUVmax average = 7.7), and compared to a
small proportion of patients demonstrating muscular
Weber (2004) reports that non-shivering
uptake (SUVmax average = 5.8) within the same
thermogenesis is triggered by the sympathetic
region. These similar figures indicate that it may be
nervous system, in response to cold temperatures.
difficult to assess the difference between 18F-FDG
Norepinephrine is released and binds to the β3-
accumulation in BAT and muscle and further
adrenergic receptors on the BAT cell surface
emphasise the benefit of anatomical localisation
causing enzyme action, which in turn begins the
provided by PET/CT.
heat production process. Glucose transport is also
initiated by the release norepinephrine. Glucose
In a similar analysis, of the 359 patients who
transporter 1 (GLUT1) and glucose transporter 4
underwent PET/CT, 49 patients (14.1%) were found
(GLUT4) are primarily involved and it is the
to have abnormal 18F-FDG accumulation within the
activation of these glucose transporters by which
supraclavicular area (Cohade, Osman, et al., 2003).
18F-FDG uptake into BAT is mediated (Nedergaard,
Abnormal tracer accumulation was compared to
et al., 2007; Weber, 2004).
corresponding tissue on the CT images with the CT
tissue densities used to delineate between fat, muscle
Brown Adipose Tissue on 18F-FDG PET
and lymph tissue (Fat density -75.9 ± 24 HU, Muscle
PET/CT imaging has been used extensively to
31.9 ± 14 HU and lymph tissue 29.8±12 HU
correctly localise areas of normal 18F-FDG
(Cohade, Osman, et al., 2003)). Results demonstrated
accumulation to anatomical structures. Several
14 patients with BAT accumulation. No statistically
analyses have been performed, all supporting the
significant difference was found between the BMI or
claim that areas of increased BAT accumulation are
the age of patients that demonstrated hypermetabolic
due to hypermetabolic BAT. Hany, et al. (2002)
BAT when compared to those that demonstrated
performed an investigation of 638 consecutive
muscular or lymph tissue uptake. A comparison was
patients who underwent PET/CT and reported
made between the SUVmax for BAT, muscle and
increased symmetrical 18F-FDG accumulation
lymph tissue. The SUVmax of muscle was
within the shoulder area in 17 patients (2.5%).
significantly lower than that of lymph tissue and
PET/CT localised this accumulation to the fatty
BAT (Cohade, Osman, et al., 2003). These findings
tissue of the shoulders in all patients. Two distinct
are comparable with the SUV measurements gained
patterns of accumulation were noted: The first
in other investigations (Yeung, et al., 2003).
within the shoulder area (supraclavicular) and the
second within the neck, shoulder and thoracic spine
In the investigation of 845 performed by Truong, et
areas (neck, supraclavicular and paravertebral).
al. (2004), similar appearances of abnormal 18F-FDG
Interestingly, the latter pattern was demonstrated
uptake was found in 25 patients that correlated to
within 7 female patients. Investigators also note a
hypermetabolic BAT. Interestingly, the results
probable link between body mass index (BMI) and
indicated that there is a female predominance for the
the appearance of BAT, although no statistical
presence of BAT (Truong, et al., 2004), a finding
testing was performed. In four out of the seven
that has not been demonstrated by other investigators
patients that demonstrated the latter pattern of
(Cohade, Osman, et al., 2003; Hany, et al., 2002;
uptake the BMI was within the underweight range
Yeung, et al., 2003). However, other investigations
(<18.5), with the average BMI of all other patients
into the appearance of BAT in rodents have also
being 22.7 (Normal range was defined as 18.5-
suggested a female predominance (Nedergaard, et
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Investigators have identified and described five
incidence rate of 23.8% in patients less than 18 years
typical areas of increased 18F-FDG accumulation
of age was demonstrated, compared to 5.9% in
that can be localised to BAT through the use of
patients over the age of 18.
PET/CT. Of these five areas, it appears more
common to find hypermetabolic BAT within the
A similar investigation by Kim, et al. (Kim,
supraclavicular and neck areas, when compared to
Krynyckyi, Machac, & Kim, 2008) analysed 1495
the mediastinal, paravertebral and suprarenal areas.
PET scans that were performed in 1159 patients (566
There is evidence to suggest that female patients are
men, 593 women and 22 patients less than 18 years
more likely to demonstrate hypermetabolic BAT,
of age). 42 scans were found to be positive for
when compared to their male counterpart. As it is
hypermetabolic BAT. A higher incidence was once
known that younger members of the population
again demonstrated within patients less than 18 years
have BAT, it is not surprising that investigations
of age, with an incidence of 13.6% compared to that
show that hypermetabolic BAT is of a higher
of the adult population at 2.8%. A comparison was
proportion within the paediatric population,
made between the incidence of hypermetabolic BAT
compared with adults. Only limited evidence exists
to the outdoor temperature on the day of PET
that the appearance of hypermetabolic BAT is
imaging, and 2, 3, 7, 14, 30 and 60 days prior to
related to BMI, with some investigations suggesting
imaging. BAT appearance was found to be more
that patients with a lower BMI are more likely to
common when the outdoor temperature was lower on
demonstrate BAT. Similar SUVs have been
the day of the scan and up to a week prior.
obtained for BAT, muscle and lymph tissue, which
Incidences were more common during the winter
places emphasis on the importance of PET/CT
months. There was no significant relationship
anatomical localisation to delineate between the
demonstrated between the appearance of BAT and
three tissue types.
the temperature 14, 30 and 60 days prior to the PET
scan. Kim, et al. (2008) concluded that the
In addition to sex and age, the two main causes of
appearance of BAT was more likely as a
hypermetabolic BAT on PET/CT are environmental
consequence of exposure to acute cold conditions,
temperature and diet (Nedergaard, et al., 2007). Of
rather than as a result of prolonged cold exposure as
the investigations studied, it is unlikely that diet has
proposed by Cohade, Mourtzikos, et al. (2003). As
had any effect on the activation of BAT. All patients
CT localisation was not available during this
were fasted for a period between four and six hours
investigation, Kim, et al. relied upon the knowledge
prior to the administration of 18F-FDG. In trusting
that BAT is found in several common locations to
that all patients had fully complied with preparation
interpret and assess their PET scans. Whilst this
instructions, this effectively eliminates patient diet
method cannot be regarded as accurate as Cohade,
as a probable cause for hypermetabolic BAT. It is
Mourtzikos, et al.‟s (2003) for the determination of
more likely that the environmental temperature of
BAT appearance, and consequently, the influence
the patients prior to administration and during the
that outdoor temperature has on BAT; the findings of
uptake period of 18F-FDG has resulted in BAT
the study are considerable.
Despite the evidence from Cohade, Mourtzikos, et al.
The effect of cold exposure on FDG distribution
(2003) and Kim, et al. (2008) that cold exposure,
Cohade, Mourtzikos,et al. (Cohade, Mourtzikos, &
whether it be acute or prolonged, can cause BAT
Wahl, 2003) performed a retrospective analysis of
appearance of 18F-FDG PET there is limited
1017 PET/CT scans and compared those that
literature on the topic. The most probable cause for
demonstrated BAT with the outdoor temperature.
the lack of investigations are the ethical
BAT was identified in 68 patients (6.7%), with 11
considerations surrounding humans undergoing PET
being male and 52 being female. The incidence of
for research purposes only, and it is difficult to
the appearance of BAT was compared with the
justify their unnecessary radiation exposure. Two
outdoor temperature during the month of the
groups of investigators have conducted studies using
patients scan, and one, two and three months prior
simulated cold environments in attempt to reproduce
to the month of the scan. Cohade, Mourtzikos, et al.
the appearance of hypermetabolic BAT.
(2003) deduced that the occurrence of BAT is more
likely to occur in the month‟s directly succeeding
Baba, et al. (Baba, Engles, Huso, Ishimori, & Wahl,
the onset of winter (February and March: Study
2007) conducted an investigation to assess the
completed in Northern Hemisphere), (Cohade,
appearance of multiple radiotracers in BAT at room
Mourtzikos, et al., 2003). In turn, it may be possible
temperature and cold environments, using rats at
that the appearance of hypermetabolic BAT on 18F-
their subject. 18F-FDG was injected intravenously
FDG is due to the activation of BAT due to
into two groups of rats, the first group exposed to
prolonged cold exposure, rather than as a
22.5°C for four hours prior to injection, and the
consequence of direct cold exposure. Additionally,
second exposed to 4°C for the same time. One hour
Cohade, Mourtzikos, et al.‟s investigation further
post injection, the rats were sacrificed; interscapular
emphasised that BAT appearance is more likely to
BAT extracted, assessed under microscope and
be encountered in the paediatric population. An
measured for the presence of 18F-FDG. Baba et al.
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
(2007) determined that there was a statistically
occurrence which initially led researchers to believe
significant increase (26 times greater; P < 0.01) in
that what we now understand to be BAT, to be
the presence 18F-FDG in BAT for the cold exposed
muscle uptake in anxious patients (Yeung, et al.,
rats, when compared to the control group. This
2003). Despite this, there has been limited success
study effectively demonstrates that acute cold
using diazepam for this purpose. Gelfand, et al
exposure can induce 18F-FDG presence in BAT.
(Gelfand, O'Hara, Curtwright, & MacLean, 2005)
Despite this, the conditions represented within the
performed 118 PET scans in 69 paediatric patients
investigation can be considered „extreme‟, and it is
(average age was 12.9 years of age, 76 male and 42
unlikely that patients would encounter similar
female). In 88 studies, premedication was
conditions prior to routine PET scanning.
administered. 44 patients received intravenous
The most relevant investigation into the effect of
fentanyl (dose 0.75-1 μg/kg), 34 received oral
cold exposure on the appearance of 18F-FDG in
diazepam at a dose of 0.06mg/kg and 9 received
BAT has been conducted by van Marken
0.10mg/kg. 29.4% of patients who received low
Lichtenbelt, et al. (van Marken Lichtenbelt, et al.,
dose diazepam demonstrated BAT and of the patients
2009). 24 healthy male patients were investigated
that received fentanyl only 6.7% demonstrated BAT.
(10 with a BMI <25 and 14 with a BMI 25) with
Of the patients that received no premedication,
18F-FDG during exposure to mild cold (16°C). Prior
26.1% demonstrated BAT. None of the patients that
to PET/CT imaging, all subjects were fasted for the
received moderate dose diazepam demonstrated
same duration and wore standardised clothing. The
BAT, but it is likely that the result may be skewed
subjects were placed in a climate chamber for 1
due to a small sample size. No difference was
hour at 22°C and were then exposed to cold
reported between male and female patients and those
conditions at 16°C for a further two hours. After the
that received low dose oral diazepam and those that
first hour of cold exposure the subjects were
received no premedication. Although Gelfand, et al.
administered 74MBq of 18F-FDG intravenously.
(2005) demonstrated that the administration of
PET/CT scanning occurred after the second hour.
fentanyl was able to reduce the incidence of BAT
Three of the subjects were then re-evaluated using a
they did not report complete effectiveness.
constant temperature of 22°C. 23 patients were
confirmed to have hypermetabolic BAT on PET/CT
Jacobsson (Jacobsson, Bruzelius, & Larsson, 2005)
to varying degrees with the exception being one
reported the use of propranolol was successful in
subject with a BMI of 38.7 - the highest BMI of all
reducing the appearance of BAT. A male patient who
subjects. A higher amount of BAT was
underwent a PET examination was reported to have
demonstrated in subjects with a lower BMI in
extensive BAT that could not be distinguished from
keeping with the findings of previous investigations
actual disease. The patient underwent a repeat
(Hany, et al., 2002), although no statistically
examination 3 weeks later following the oral
significance difference was reported. There was no
administration of 80mg of propranolol. Jacobsson, et
BAT observed within the patients that underwent
al. (2005) reported a compete resolution of the
re-evaluation at 22°C. The investigation by van
hypermetabolic BAT. Following Jasobsson, et al.‟s
Marken Lichtenbelt, et al. (2009) depicts similar
(2005) revelation several groups of investigators
conditions that may be encountered during routine
have conducted studies into the use of propranolol as
PET scanning when compared to that of Baba, et al.
an effective means of preventing hypermetabolic
(2007). Although there is this discrepancy, the
BAT on 18F-FDG PET.
conclusions of both investigations are similar and
both demonstrate the effect that cold exposure has
Soderlund (Soderlund, Larsson, & Jacobsson, 2007)
on 18F-FDG imaging and confirm the presence of
investigated 11 patients that were reported to have
hypermetabolic BAT.
BAT on their PET scans by performing a second
examination 5 days post the first PET study. Prior to
Reduction of BAT on 18F-FDG PET
the administrated of 18F-FDG the patients were given
Recently, the majority of investigators have focused
80mg of propranolol orally. All patients showed a
on the administration of pharmaceuticals with the
complete or almost complete disappearance of BAT
attempt of reducing the appearance of BAT on
on the second PET examination (P< 0.001)
18FDG PET. These pharmaceuticals include
(Soderlund, et al., 2007). Disease that was present
propranolol; a β-blocker and diazepam; a
with some of the patients on their first PET scan
benzodiazepine and fentanyl; an opiate. Other
remained unchanged, suggesting that the oral
methods reported have included controlling the
administration of propranolol prior 18F-FDG does not
environmental temperature of the patient and
alter the biodistribution within tumours. Soderlund,
controlling the diet of the patient. All techniques
et al. (2007) also reported that propranolol had the
have varying reports of success in reducing the
ability to reduce cardiac uptake of 18F-FDG,
appearance of BAT.
although the difference was not significant.
Agrawel (Agrawal, et al., 2009) reported a similar
Diazepam was the first pharmaceutical to show
success rate in the reduction of hypermetabolic BAT
effectiveness in reducing BAT appearance - an
following the administration of propranolol. 40
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
patients (14 females and 26 males) who
the effectiveness of controlling the temperature of
demonstrated BAT on an initial PET scan were re-
the patients environment prior to 18F-FDG
examined following the oral administration of 40mg
administration has been under investigated.
of propranolol. The repeat PET scan was repeated
48 hours post the initial scan, and the propranolol
Christensen, et al. (Christensen, Clark, & Morton,
was administered 60 minutes prior to 18F-FDG.
2006) proved that by attempting to control the
Patients taking β-blockers were excluded from the
patients environmental temperature prior to 18F-FDG
study. 90% of patients demonstrated a complete
injection, hypermetabolic BAT could be reduced just
clearance of 18F-FDG from BAT on their second
as effectively as with the administration of
PET scan. Agrawel, et al. (2009) suggest that the
propranolol. During the investigation, 10 patients
BAT observed in 10% of patients may have been
were selected that had previously demonstrated BAT
due to the external influences on hypermetabolic
on their PET scan. 3 patients were provided with
BAT such as anxiety level, temperature and blood
warm blankets from a blanket oven during the uptake
glucose level; as these factors were not controlled
period, 4 patients were instructed to stay in a warm
during the investigation.
environment for 48 hours prior to their scan and 3
patients were instructed to stay in a warm
Parysow (Parysow, et al., 2007) also investigated
environment for 48 hours prior to their scan and
the effectiveness of oral propranolol and reported a
given 5mg of oral diazepam at the time of 18F-FDG
similar success rate as Agrawel, et al. (2009) and
injection ((Christensen, et al., 2006). Patients
Soderlund, et al. (2007). 26 patients that had been
underwent PET/CT at 60mins following injection.
previously identified at having hypermetabolic BAT
All but one patient (90%) showed complete
on PET were administered 20mg of oral propranolol
resolution of hypermetabolic BAT on their second
60mins prior to 18F-FDG. 24 patients (92.3%)
scan. This success rate in the reduction of BAT is
demonstrated no BAT after being administered with
comparable with that achieved using propranolol,
the propranolol. The remaining 7.69% of patients
although the sample size within this study is small.
still demonstrated BAT, although the distribution
In a similar sized study Garcia, et al. (Garcia, et al.,
and SUVmax was reduced, but not significantly.
2006) re-evaluated 10 patients who were reported to
have hypermetabolic BAT on an initial PET scan.
Tatsumi (Tatsumi, et al., 2004) conducted an
Patients were instructed to wear warm winter-type
extensive investigation using rats, similar to that of
clothing prior to their scan and during transit from
Baba, et al. (2007). Three groups of rats were
home to the PET centre and pre-warm their car‟s
anaesthetised and each of the groups were
interior to room temperature. Upon arrival to the
administered propranolol, diazepam or reserpine (an
PET centre, patients were placed in a temperature
antihypertensive) intraperitoneally post anaesthesia.
controlled room and provided with warm blankets.
The dose administered were 5mg/kg of propranolol
Warm blankets were also provided during the uptake
20mins prior to 18F-FDG, 4mg/kg of reserpine 4 h
period. Four observers assessed the PET scans for
prior to 18F-FDG, and 2.5mg/kg of diazepam 30min
any presence of hypermetabolic BAT and reported
prior to 18F-FDG. A control group was also included
no BAT visualisation in 70-90% of patients
and received no medication prior to 18F-FDG. 60
(allowing for inter-observer variability).
minutes following 18F-FDG injection, the rats were
sacrificed, interscapular BAT removed and
Both Christensen, et al. (2006) and Garcia, et al.
examined under microscope and measured for the
(2006) have reported a high level of success (70-
presence of 18F-FDG. Tatsumi, et al. (2004)
90%) in reducing hypermetabolic BAT on 18F-FDG
demonstrated propranolol to be the most effective
PET through simply attempting to control the
medication in reducing the 18F-FDG uptake in BAT,
patients environmental temperature prior to their
reducing it to just 16% of the control value.
scan. These figures are despite small sample sizes
and are comparable with that achieved using
Reserpine was also effective, reducing BAT activity
pharmaceuticals such as propranolol. Surprisingly,
to 28% of the control. Diazepam was also effective
despite a similar success rate there have been limited
in reducing the 18F-FDG uptake in BAT, but the
investigations into the use of warming techniques.
result was not statistically significant, achieving
only a 64% reduction when compared to the control.
Conclusion
The administration of propranolol one hour prior to
Hypermetabolic BAT, when present, has the
the administration of 18F-FDG has been
potential to reduce the accuracy of 18F-FDG PET.
demonstrated at the most effective pharmaceutical
Whenever possible, an attempt must be made to
in reducing the incidence of hypermetabolic BAT
reduce its appearance. Hypermetabolic BAT has
on PET. The reported success rate is approximately
been visualised in all types of patients but a higher
90% (Agrawal, et al., 2009; Parysow, et al., 2007;
incidence has been observed in female patients, the
Soderlund, et al., 2007; Tatsumi, et al., 2004).
paediatric population and those patients with a low
Given the evidence that there is a strong relationship
BMI. The appearance of BAT appears to be as a
between temperature exposure and BAT appearance
consequence of the environmental temperature of the
(Cohade, Mourtzikos, et al., 2003; Kim, et al., 2008)
patient prior to their PET scan. Pharmaceutical
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
intervention has proven to be successful in reducing
to patients does not come without risks or the need to
the appearance, with oral propranolol proving the
manage outpatients following administration. The
most successful. Several small studies into
use of warming techniques comes with relative ease
environmental temperature control prior to scanning
when compared to pharmaceutical intervention and
have demonstrated a similar success. Although
there is a need to conduct further investigations to
highly effective, the administration of propranolol
emphasise their effectiveness.
REFERENCES
Agrawal, A., Nair, N., & Baghel, N. S. (2009). A novel approach for reduction of brown fat uptake on FDG PET. [Journal Article]. The British Journal of Radiology, 82, 626-631.
Baba, S., Engles, J. M., Huso, D. L., Ishimori, T., & Wahl, R. L. (2007). Comparison of Uptake of Multiple Clinical Radiotracers into Brown Adipose Tissue under Cold-Simulated and Nonsimulated Conditions. [Journal Article]. J Nuclear Medicine, 48, 1715-1723.
Celi, F. (2009). Brown Adipose Tissue - When it Pays to Be Inefficient. [Journal Article]. New England Journal of Medicine, 306(15), 1553-1556.
Christensen, C. R., Clark, P. B., & Morton, K. A. (2006). Reversal of Hypermetabolic Brown Adipsoe Tissue in F-18 FDG PET Imaging. Clinical Nuclear Medicine, 31(4), 193-196.
Cohade, C., Mourtzikos, K. A., & Wahl, R. L. (2003). "USA-Fat": Prevalence Is Related to Ambient Outdoor Temperature - Evaluation with 18F-FDG PET/CT. [Journal Article]. J Nuclear Medicine, 44, 1267-1270.
Cohade, C., Osman, M., Pannu, H. K., & Wahl, R. L. (2003). Uptake in Supraclavicular Area Fat ("USA-Fat"): Description on 18F-FDG PET/CT. [Journal Article]. J Nuclear Medicine, 44, 170-176.
Cypess, A. M., Lehman, S., Williams, G., Tal, I., Rodman, D., Goldfine, A. B., et al. (2009). Indentification and Importance of Brown Adipose Tissue in Adult Humans. New England Journal of Medicine, 360(15), 1509-1517.
Evans, K. D., Tulloss, T. A., & Hall, N. (2007). 18FDG Uptake in Brown Fat: Potential for False Positives. [Journal Article]. Radiologic Technology, 78(5), 361-366.
Garcia, C. A., Nostrand, D. V., Acio, A. E., Bulter, C., Esposito, G., Kulkarni, K., et al. (2006). Reduction of Brown Fat 2-Deoxy-2-[F-18] fluoro-D-glucose Uptake by Controlling Environmental Temperature Prior to Positron Emission Tomography Scan. Molecular Imaging and Biology, 8, 24-29.
Gelfand, M. J., O'Hara, S. M., Curtwright, L. A., & MacLean, J. R. (2005). Pre-medication to block [18F]FDG uptake in the brown adipose tissue of pediatric and adolescent patients. Pediatric Radiol, 35, 984-990.
Hany, T. F., Gharehpapagh, E., Kamel, E. M., Buck, A., Himms-Hagen, J., & von Schulthess, G. K. (2002). Brown adipose tissue: a factor to consider in symmetrical tracer uptake in the neck and upper chest region. European Journal of Nuclear Medicine, 29(10), 1393-1398.
Jacobsson, H., Bruzelius, M., & Larsson, S. A. (2005). Reduction of FDG upatke in brown adipose tissue by propranolol. Eur J Nucl Med Mol Imaging, 32, 1130.
Kim, S., Krynyckyi, B. R., Machac, J., & Kim, C. K. (2008). Temporal relation between temperature change and FDG uptake in brown adipose tissue. Eur J Nucl Med Mol Imaging, 35, 984-989.
Nedergaard, J., Bengtsson, T., & Cannon, B. (2007). Unexpected evidence for active brown adipose tissue in adult humans. Am J Physiol Endocrinol Metab, 293, E444-E452.
Paidisetty, S., & Blodgett, T. M. (2009). Brown Fat: Atypical Locations and Appearances Encountered in PET/CT. AJR, 193, 359-366.
Parysow, O., Mollerach, A. M., Jager, V., Racioppi, S., Roman, J. S., & Gerbaudo, V. H. (2007). Low-Dose Oral Propranolol Could Reduce Brown Adipose Tissue F-18 FDG Uptake in Pateints Undergoing PET Scans. Clinical Nuclear Medicine, 32, 351-357.
Soderlund, V., Larsson, S. A., & Jacobsson, H. (2007). Reduction of FDG Uptake in brown adipose tissue in clinical patients by a single dose of propranolol. Eur J Nucl Med Mol Imaging, 34, 1018-1022.
Tatsumi, M., Engles, J. M., Ishimori, T., Nicely, O., Cohade, C., & Wahl, R. L. (2004). Intense 18F-FDG Uptake in Brown Fat Can Be Reduced Pharmacologically. J Nuclear Medicine, 45, 1189-1193.
Truong, M. T., Erasmus, J. J., Munden, R. F., Marom, E. M., Sabloff, B. S., Gladish, G. W., et al. (2004). Focal FDG Uptake in Mediastinal Brown Fat Mimicking Malignancy: A Potential Pitfall Resolved on PET/CT. AJR, 183, 1127-1132.
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
van Marken Lichtenbelt, W. D., Vanhommerig, J. W., Smulders, N. M., Drossaerts, J. M. A. F. L., Kemerink, G. J., Bouvy, N. D., et al. (2009). Cold-Activated Brown Adipsoe Tissue in Healthy Men. New England Journal of Medicine, 360(15), 1500-1508.
Virtanen, K. A., Lidell, M. E., Orava, J., Heglind, M., Westergren, R., Niemi, T., et al. (2009). Functional Brown Adipose Tissue in Healthy Adults. New England Journal of Medicine, 360(15), 1518-1525.
Weber, W. A. (2004). Brown Adipose Tissue and Nuclear Medicine Imaging. J Nuclear Medicine, 45(7), 1101-1103.
Williams, G., & Kolodny, G. M. (2008). Method for Decreasing Uptake of 18FDG by Hypermetabolic Brown Adipose Tissue on PET. AJR, 190, 1406-1409.
Yeung, H. W., Grewal, R. K., Gonen, M., Schoder, H., & Larson, S. M. (2003). Patterns of 18F-FDG Uptake in Adipose Tissue and Muscle: A Potential Source of False-Positives for PET. J Nuclear Medicine, 44, 1789-1796.
Continuing Professional Development – Question and Answer Sheet
Article title: Brown Adipose Tissue and 18F-FDG PET. Your name:
RAINS Member Number: _ Answer the following questions and return the completed sheet before the middle of the month to: RAINS
Charles Sturt University
[email protected]
Wagga Wagga NSW 2678
1). Initially, the appearance of BAT was thought to be what? 2). What are the five common locations of BAT? 3). What are the unique characteristics of BAT? 4). How does 18F-FDG localise in BAT? 5). Describe some characteristic s of a patient that may be more likely to have activated BAT on 18F-FDG PET. 6). Describe the relationship between temperature and the incidence of BAT. 7). What is the proposed action by which the administration of propranolol appears to block the appearance of BAT on 18F-FDG PET? 8). Soderlund, et al. (2007) administered 80mg of propranolol to patients prior to their PET scan. What was their success rate in reducing the appearance of BAT? 9). What effective technique that can be utilised in the reduction of BAT on 18F-FDG PET has been under-investigated?
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Crossword Puzzles
The ANZSNM is now accepting a broader variety of CPD activities. Crossword puzzles now attract 1 CPD point
when completed. You are not required to submit them for marking. The CPD requirements of the ANZSNM
simply require that you record in your CPD diary that a CPD activity was undertaken. This has been confirmed
in writing by the ANZSNM. So complete the crosswords below (and other CPD activities) and record these
activities in your diary as proof in the event that you are audited.
Submit your crossword. You can use the free puzzle maker at
Save the puzzle and solutions as a webpage and send to [email protected]
Charles Sturt University.
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Radiopharmacy Clues
3 Approximate half life of 99Tc hours
1 How 99Mo is produced
6 Approximate half life of 11C minutes
2 67Ga radiochemical gallium _
7 Principle of radiation safety
4 Approximate half life of 13N minutes
10 Transition metal that is element 43 on periodic
5 Method of disposal of 99mTc waste; decay by
8 The 'm' in 99mTc
11 Half lives required to decay to 'background'
9 System imaged using mertiatide
12 'D' in TDS
13 How 89Sr is produced activation
15 18F based dopamine receptor tracer
14 Type of equilibrium for the Mo/Tc generator
17 201Tl produced in a _
16 Imaged with medronate
20 'S' in TDS
18 System imaged with 99mTc disofenin
23 Decay constant
19 201Tl radiochemical thallous _
24 'T' in TDS
21 'G' in FDG
25 Generator based PET blood flow agent 82-
22 More common abbreviated name fro exametazime
27 Approximate half life of 15O minutes
26 Where 99Mo is produced
1 Positron emission tomography
2 Ethane-1-hydroxy-1, 1-diphosphonate
3 Magnetic resonance imaging
5 As low as reasonably achievable
8 Diethylenetriamine pentaacetic acid
6 Region of interest
9 Not for resusitation
8 Digital imaging and communications in medicine
12 Rural alliance in nuclear scintigraphy
10 Mini-mental state examination
11 Meta-iodobenzylguanidine
18 Hydroxymethan diphosphonate
13 Carcinoembryonic antigen
14 O-(2-[18F]fluoroethyl)-L-tyrosine
25 Roentgen absorbed dose
27 Prospective investigation of pulmonary embolism 16 [18]F-3'-deoxy-3'-fluorothymidine
19 Counts per minute
30 Pulomonary embolism
22 Coronary artery disease
31 Methylene diphosphonate
32 Dimercaptosuccinic acid
24 Blood pressure
33 Radiology information system
26 Australian and New Zealand society of nuclear
35 Gastrointestinal tract
29 Alzeimer's disease
38 Chronic obstructive pulmonary disease
34 Single photon emission computed tomography
40 Heart rate
36 Bismuth germinate
41 Fluorine-18 2-fluoro-deoxyglucose
38 Cerberal blood flow
43 Myocardial infarction
39 Neck of femur
46 Ethyl cysteinate dimer
40 Hexamethylpropyleneamine oxime
47 Statim (immediately)
42 Glioblastoma multiforme
48 Monoclonal antibody
43 Methoxy isobutyl isonitrile
44 Ethylene-diamine-tetra-acetic acid
45 Picture archiving and communication system
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Charles Sturt University.
Submit your crossword. You can use the free puzzle maker at
Save the puzzle and solutions as a webpage and send to [email protected]
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Musculoskeletal Gross Anatomy
Charles Sturt University.
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Musculoskeletal Gross Anatomy Clues
1 Finger and toes
2 Bum muscle (7,7)
3 Abdominal muscle (6,9)
4 C2 spine
8 Calf muscle
5 Upper jaw
10 Forearm bone
6 Lower leg muscle
12 Shoulder muscle
7 Carpal bone (l )
13 C1 spine
9 Hip bone
14 Pelvic based section of spine
11 Lower leg bone
15 Spine region of rib attachment
18 Chest muscle
16 Midfoot bone
19 Lower jaw
17 Thigh muscle
20 Carpal bone (p )
21 Upper arm bone
23 Bones of the wrist
22 Heel bone
24 Shoulder girdle
26 Irregular midfoot bones
25 Sub unit of spine
27 Tip of spine
29 Pelvic bone
28 Upper arm muscle
30 Region of upper spine
33 Carpal bone (s _)
31 Knee bone
34 Lower non fused spine region
32 Upper arm muscle
35 Carpal bone (c _)
36 Skull bones
40 Collar bone
37 Forearm bone
41 Bones of the ankle
38 Carpal bone (h )
42 Midfoot bone
39 Bones protecting the chest contents
43 Bone of the hind foot
41 Lower leg bone
44 Midline pelvic bone
45 Breast bone
46 Upper leg bone
Crossword Puzzle Challenge
The crossword puzzle offers a very efficient tool for gaining CPD
points. It does not take long to create. The puzzles below were team
efforts from the respective departments and the authors (and their
departments) issue a challenge to other nuclear medicine
departments to form a team and create a better crossword puzzle for
the next newsletter. There should, however, be some ground rules.
Firstly, the crossword needs to be on a specific theme (eg. PET,
GIT imaging, SPECT/CT etc) not just general nuclear medicine.
Secondly, the puzzle needs to contain between 30-40 clues. Submit
your department crossword for the next edition of the newsletter.
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
PRP Diagnostic Imaging Team Effort
3 The bone of insertion of the Achilles tendon.
1 Primary malignant tumour of bone whose cells
4 Pathology indicated if myocardial perfusion at
produce hyaline cartilage resulting in abnormal
rest is normal while the stress shows an area of
cartilage and - or bone.
decreased perfusion.
2 The medical term for the symptom of difficulty
6 Type of ultrasound used to diagnose DVT.
9 Liver mass detected on a Tc-RBC scan.
5 Process of separating blood.
12 Most likely cause of fractures.
7 imaging: A technique used in
13 Isotope used for bone palliation.
myocardial perfusion imaging to correct for
15 Likely pathology demonstrated on Bone scan
diaphragmatic attenuation.
as hot spots in the ribs which appear to be in a
8 What does the E stand for in VEB in relation to
16 Increased alkaline phosphate is an indicator for
10 Term used to describe a WB bone scan
which common bone pathology.
showing diffusely increased bony uptake with
17 Interventional drug commonly used in renal
absent or near complete absence of soft tissue,
imaging for PUJ obstruction.
renal, and bladder tracer activity.
11 Initials for the agent used in
lymphoscintigraphy.
14 Pharmaceutical used in evaluating loss of or
decrease blood supply in cerebral perfusion
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Nuclear Medicine
Toowoomba Nuclear Imaging.
1 Nuc med techs always work _?
1 Antibody response
2 Haemangiomas are deficient in these cells
3 Neural crest tumour
5 Spinal joint
4 Liver-spleen mechanism of uptake
6 Needed to reduce pertechnetate prior to tagging
5 A response which occurs following Metastron
7 Mechanism of lung perfusion
10 Tl-201 is a potassium ?
radiopharmaceutical localisation.
11 Time magazines year 2000 invention of the
8 PET pharmaceutical
13 Bone scan agent
9 Conceived the tracer principle
14 Autoimmune condition
12 Early bone imaging agent
16 DMSA (dimercaptosuccinid _)
15 Treated with P32
17 Imaged with MIBG
18 Pelvic bone
19 Required in Gallium localisation
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
MASTER OF MEDICAL RADIATION SCIENCE
Flexible delivery entirely by distance education.
May attract higher award wages.
Contributes to CPD.
Update your qualifications to match the new postgraduate technologists.
Generic Master of Medical Radiation Science for 100% coursework.
Nuclear Medicine specialisation for a mix of coursework and research project.
Applications made directly to the University.
For details visit www.csu.edu.au.
Course Coordinator
Specialisation Coordinator
Master of Medical Radiation Science
Nuclear Medicine
Email: [email protected]
Email: [email protected]
Tel: 02 6933 2500
Tel: 02 6933 2822
Other study options include:
CT for Nuclear Medicine (NMT415) – associate subject or elective in the
Masters – approved by NSW EPA for SPECT/CT and PET/CT licence.
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
What The ……. ?
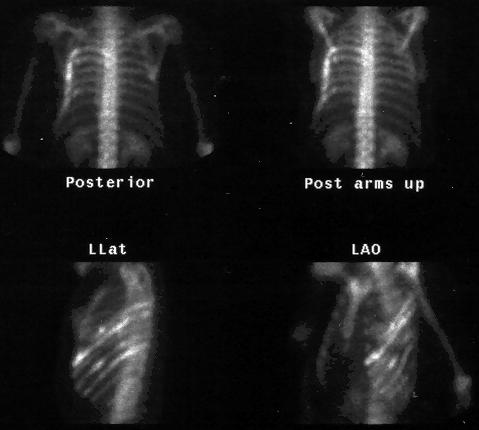
Charles Sturt University. Chest statics from a wholebody bone scan. Solution in the next issue.
Send your ‘What The …… ?' image, solution and author details to
[email protected]
What The ….? Solution For Last Edition
Monostotic Paget‟s disease of the heel
RAINS CPD Initiatives.
The following initiatives have been developed by RAINS to facilitate achievement of the 30 CPD points for RAINS members. These are proposed activities that mirror activities approved by the ANZSNM with some modification for more ready use in the rural environment.
Activity
Description
CPD Points
RAINS members can submit a power point presentation of one or more clinical
2 presenter points
cases. Content should include patient history, scan methodology, other imaging
procedures, relevant technical information, final report and patient outcomes of 20-
1 attendee point
View, read and submit review questions (80% pass mark).
Continuing Education
Each issue of Seasonal RAINS will contain 1 or more continuing education articles
Articles and Tests
with tests. Completion of the tests and submission back to RAINS with an 80% pass mark will attract CPD points.
Writing CPD articles/tests
RAINS members are encouraged to write fully referenced and scientific continuing
education articles accompanied by 10 „test‟ questions and submit for distribution in
Short Courses and
CSU in conjunction with RAINS and the ACT Branch of the ANZSNM organise
an annual 2 day CE workshop in Wagga.
In-service Education
Provide 30 minute power point presentation with narration for inclusion on CPD
CD, including written question).
View, read and submit review questions (80% pass mark).
Book / journal review
Write a considered book review (nuclear medicine) or journal article review for
inclusion in Seasonal RAINS (1 page).
Professional Development
RAINS will develop and circulated a professional development plan template for
members wishing to use it.
Complete the crossword and make a notation in your CPD diary.
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
The Doctor of Health Science
Introduction
The Doctor of Health Science (DHlthSc) at CSU is a
professional doctorate that allows candidates to pursue
a research higher degree of the same standard as the
PhD but within a structure that is aimed at improving
professional practice. Specifically, it offers a research
based approach for provision of solutions relevant to
the professions and industry.
Professional doctorates aim to provide a tool for
advanced research enabling candidates to contribute in
a significant way to the knowledge and practice in
their profession or discipline area. Consequently,
Admission Requirements
candidates enrolled in professional doctorates tend to
For admission to the DHlthSc applicants would need to
be more intrinsically motivated aiming to improve
demonstrate that they:
professional practice and enhance job satisfaction.
are working in an appropriate field within, or
relevant to, the Health Professions and can
Course Structure
demonstrate they have the opportunity and
The DHlthSc is offered by part-time distance
facilities to complete the applied
education mode and is composed of coursework and
research/investigation components of the
an applied research/professional component. Student‟s
progress through the research/professional component
have had a minimum of 3 years of relevant
of the DHlthSc is monitored by the requirement that
professional and/or vocational experience
students complete subjects in sequence thus meeting
(with relevance being determined by the
pre-defined milestones. The applied
DHlthSc Course Coordinator in conjunction
research/investigation allows students to develop a
with the proposed principal supervisor); and
research question or topic for investigation by
normally hold a Masters degree or equivalent
conducting an intensive literature review, critique and
(by coursework) in an approved area of Health
reflecting on their professional practices.
Sciences, with credit grades or above in all
subjects undertaken.
The DHlthSc culminates in a professional portfolio
(including an exegesis), which integrates the
Course Aims and Objectives
research/investigation within their professional
The DHlthSc promotes an advanced, critical reflection
practice. The professional portfolio incorporates
on professional practice in the health sciences and aims
reports, papers and publications prepared throughout
the course with an exegesis to link the results back to
provide opportunity for the candidates to
the profession and professional practice, and original
continue lifelong learning in keeping with the
question on which the research or investigation is
university‟s mission statement;
based. The professional portfolio with exegesis is
satisfy the educational needs of professionals
subjected to external examination in accordance with
working in or aspiring to work in the most
University regulations.
senior tiers of the health sciences and related
The duration of the DHlthSc is the equivalent of 4.5
promote the acquisition of advanced analytical
years part time enrolment.
and problem solving skills and conceptual
insights that enhance the capacity of the
Enrolment Pattern
candidate to undertake positions of significant
HSC700 Research Critique and Publication
responsibility in the health sciences;
HSC701 Reflective Practice in Health Science
encourage excellence in scholarship and
HSC702 Proposal For Applied Research
focused research within the candidates
HSC703 Research Project and Report 64 Points
discipline area.
HSC704 Health Science Portfolio / Exegesis
Course Coordinator
For all inquiries please contact info.csu on:
Dr Janelle Wheat
Telephone: 1800 334 733 (free call within Australia)
Senior Lecturer, Faculty of Science
Telephone: 61 2 6338 6077 (outside Australia)
Telephone: 61 2 69332750
Email: [email protected]
Email: [email protected]
Web inquiry: www.csu.edu.au/student/contact
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Guidelines for Submissions to Seasonal RAINS
Seasonal RAINS will accept a number of types of
In-Service Education
submissions. All work must be written in English
Seminars should be submitted as power point
and submitted in Microsoft Word. All submission
presentations with audio narration. Audio recordings
must be accompanied by a cover letter (email is
should be embedded in the power point presentation
sufficient) indicating the type of submission, details
(not linked) using a radio quality setting (22kHz, 16
of authors and departments, contact details of the
bit, mono). Ensure sound quality is suitable for
corresponding author and a statement indicating that
circulation. Valuable presentation might only be
the submission is not subject to copyright
included if narration is re-recorded. Accepted
presentations will be included on the RAINS CPD
in-service CD. All presentations should be
All submissions will be reviewed for
accompanied by 10 review questions. Presentations
appropriateness and accuracy (where relevant).
should be sent by mail to: The Editor, PO Box U102,
Inclusion in Seasonal RAINS remains the discretion
CSU, Wagga Wagga, 2678.
of the editorial board. Preference will be given to
submissions consistent with the philosophy and purpose of RAINS.
Submissions should provide an educational review of
All submissions should be sent by email to:
an area of interest. The reviews should be well
[email protected]
researched and present all valid perspectives. CPD
articles may be accepted after review by the editorial
Letter To Editor
board. Alternatively, the submission may be accepted with some suggested revision or deemed
300-500 word limit.
not suitable for the purpose intended (CPD). All
submission must adhere to the guidelines provided
Interesting Image
by the Journal of Nuclear Medicine Technology;
1 JPG image and 300 word limit case presentation.
available on the SNM web site (www.snm.org).
CPD articles should be made available for publication without copyright authority elsewhere.
1 JPG image and 100 word limit solution.
Submitting authors accept responsibility for ensuring
News and Events
manuscripts do not breach copyright laws. Seasonal RAINS does not, however, ask that you transfer
Summary of recent or upcoming events. Update
copyright to RAINS. Thus authors are free to re-
RAINS member achievements; publication,
publish manuscripts in whole or in part in subsequent
conference presentation or scholarship.
Book or Journal Article(s) Review
Review of a recently released nuclear medicine text
Advertisement of activities, products or events
or journal article(s) related to nuclear medicine.
consistent with the philosophy and purpose of
Minimum of 1 page.
RAINS will occur without charge (including
positions vacant).
Commercial advertisements may be included at a
20-30 minute power point presentation of a relevant
cost of $100 per half page (190x125 mm landscape)
journal article in Nuclear Medicine. Submissions
and $200 per full page (190x270 mm portrait).
should include written text and discussion for each
slide plus 10 test questions.
Advertisements will not be reformatted.
Advertisements should be submitted electronically in
PDF or JPG. This is an electronic newsletter so colour is permitted at no additional cost.
Submit a 20-30 minute review summary and
presentation (power point) of one or more clinical
Advertisements should be emailed to:
cases. Content should include patient history, scan
[email protected] no later than 4 weeks prior to
methodology, other imaging procedures, relevant
technical information, final report and patient outcomes. Submissions should include written text
Start Collecting Your CPD Points
and discussion for each slide plus 10 test questions.
Copyright 2010. All rights reserved.



CENTRE FOR RESEARCH
IN COMPLEX SYSTEMS
U N I V E R S I T Y
7th Annual CPD/CME Conference: IIS2010
Stamford Grand, North Ryde
(Adjacent to Macquarie University, Sydney)
Saturday 13th & Sunday 14th November, 2010
CT MRI SPECT PET US DR/CR
The scis.
Integraonthe mod
• • • • • •
There is eythrough anatomntenters
Each sentdiagno.
The pndand CReprogram s,radiolog
CT and PET in diagnosis and management of
Transition from SPECT to PET
Medical oncology PET
Novel peptides in cancer therapy; the role of
Endocrine imaging
Coronary artery disease
PACS/RIS, ECG Tutorial or Cross sectional
PET and MRI in dementia
Pre-dinner drinks
Conference dinner
Morning tea from 1030am-11amLunch from 1230pm-130pmAfternoon tea from 3pm-330pm
Scientific Program Registration
Registration fee includes:
• All scientific program sessions
• Morning tea Saturday and Sunday
• Buffet lunch Saturday and Sunday
Early Bird
• Afternoon tea Saturday and Sunday
Conference dinner:
• 3 course buffet meal at the Stamford Grand• 3 hours of superior beverage service during dinner• 1 hour of superior beverage service at pre-dinner drinks
Note:
• Day registration includes morning tea, lunch and afternoon tea on the day of registration.
• Early bird registration discounts apply before the end of the financial year.
• CE and CPD point applications pending.
• Book accommodation directly with Stamford Grand , North Ryde using the conference discount rates of $170 for a
superior room (02 9888 1077). Executive and family suites are also available.
• Alternative accommodation can be organised at the Travelodge at Macquarie University.
• Send a RAINS membership application (free) with this form and receive the member discount (www.rains.asn.au).
Check Appropriate Box
RAINS Member before 1/7/10
Preferred Saturday workshop:
Non Member before 1/7/10
Conference Dinner (Saturday night)
Please return this form with payment (cheque or money order made payable to ‘RAINS') to:
The Secretary, RAINSPO Box U102, CSU, Wagga Wagga 2678.
Direct Deposit Payments:
Account name: RAINS
BSB: 033253Account number: 195900
Title: Surname: _ Given Name: _
Identifier: Your surname and initial
Please send completed registration form ASAP after
direct deposit, and provide the date of direct deposit
and amount.
Email (print clearly):
Please circle an appropriate descriptor: Medical Technical Nursing Scientist Other:
Please circle appropriate expertise: SPECT PET CT MRI US Therapy
Please check this box if you do not want your details made available to sponsors: □
Seas RAINS, vol. 4, no. 1
2009 Conference Report
B2B09: Back to Basics CPD Conference
Matt Ayers, RAINS President.
On the weekend of the 10/11 October, Charles Sturt
evenings festivities. The social dinner was a culinary
University and RAINS co-hosted the annual CPD
delight in the award winning resort restaurant
conference. The 'Back to Basics' theme aimed to
'surpassed' only by the unsolicited entertainment of a
discuss and disseminate knowledge and skills
number of delegates who will remain unnamed
transferable to actual clinical practice. The venue
(singing, dancing and instrument playing). Despite
was ideal at the Diamond Beach Resort near
the social activities, for many, extending into the
Forster, although the weather was disappointing.
early hours of Sunday morning, delegates faced
Sunday breakfast and session three with vigour.
Based on delegate, sponsor and committee
feedback, the weekend was an enormous success;
Prof Doug Howarth provided an enlightening
surpassing both plenary and social program
analysis of lung scintigraphy and encouragement to
all to "get off the PIOPED fence". Dr Emlyn Jones
mediated discussion on renovascular hypertension
Welcome drinks on Friday night were largely
which was absorbing. Llewelyn Clack and Melissa
prohibitive of most attending the Saturday morning
Earl presented stimulating interesting case studies.
beach Tai Chi although most managed to find their
way to the buffet breakfast. The Saturday sessions
The final session saw a riveting presentation from
commenced with Professor Hosen Kiat, who
Nathan Cassidy on breast lymphoscintigraphy and
regaled delegates with some wonderful anecdotes
sentinel node biopsy followed by an insight into
before taking us on a journey from our cardiac
making the transition from NMT to MRI
imaging roots to the latest in cardiac molecular
technologist from Coralea Kaaser and finishing with
imaging; painting an optimistic picture of the
Dr Geoff Currie presenting the pharmacological
evolving role of myocardial perfusion imaging.
basis of interventional nuclear cardiology. A
Professor Doug Howarth reminded delegates of the
scrumptious BBQ lunch followed the RAINS AGM
role and power of oesophageal transit studies and
before delegates departed well informed, well fed,
GIT bleeding scintigraphy.
and not so well rested.
Morning tea freshened the palate for an insightful
The enthusiasm of attendees and the robust
examination of bone scintigraphy and the role of
discussion generated by each of the speakers
SPECT/CT by Dr Shane Morony. Dr Emlyn Jones
highlighted the importance and relevance of the
followed with a captivating presentation of the
topics to current clinical practice.
importance of parathyroid imaging. Ian Turner from
ARI/PETNET (our major sponsors) rounded out the
The organising committee would like to extend a
session with an overview of the changing world of
warm thank you to presenters, delegates and our
Mo-99 and a comparative situation analysis between
sponsors (ARI,PetNet, InMed, GMS, Cyclomedica,
Australia and our international colleagues.
RAINS, Siemens, GE Healthcare, Insight and
Charles Sturt University,) without whom the
Lunch and an afternoon of social activities (tennis,
program could not have been achieved. We invite all
volleyball, dayspa, beach) afforded an opportunity
ANZSNM members and colleagues to participate in
to digest and discuss delivered content. InMed
kindly provided pre-dinner drinks to lubricate the
Copyright 2010. All rights reserved.
Seas RAINS, vol. 4, no. 1
Rural Alliance In Nuclear Scintigraphy - (RAINS)
APPLICATION FOR MEMBERSHIP
There are no membership fees for RAINS in 2008.
Please send complete forms to:
Or email to:
PO Box U102
Charles Sturt University
I wish to apply for membership to RAINS and, if accepted as a member, I undertake to
comply with the RAINS Charter.
See membership guidelines (please tick):
Ordinary member …………………
Associate member ………….
Professional Category (please tick): Technologist/Scientist …………….
Physician …………………….
Physicist ………………………….
Radiologist ……………………
Nurse ………………………………
Registrar ………………………
Radiopharmacist ………………….
Student Technologist (specify uni)
Other (please specify) ……….
Are you a member of (please tick): ANZSNM …………………………
AIR ………………………….
Title: _ Given Name: _ Surname: _ Business Address: _ _ Telephone: _
Email: I agree to have my telephone number and email address included on the RAINS database and circulated amongst RAINS members. Signature:
ANZSNM Member? YES / NO
Rurality Criteria Satisfied? 1 / 2 / 3 / 0
Member number issued? _
Copyright 2010. All rights reserved.
Source: http://rains.asn.au/wp-content/uploads/2014/04/seasonal_rains_v4_n1_final.pdf
Dr. med. Guy Bourgeois Dr. med. Reto Engel FMH Innere Medizin FMH Kardiologie & Innere Medizin Praxisgemeinschaft Webersbleiche, Schützengasse 2, 9000 St. Gallen Tel 071 227 40 60 Fax 071 227 40 61 Generika Wenn es Diskussionen über mögliche Kosteneinsparungen im Gesundheitswesen, insbesondere bei den Medikamenten geht, fällt schnell einmal der Begriff „Generikum". Worum handelt es sich aber dabei? Sind Generika Billigmedikamente, echte Alternativen zu teuren Originalen oder liegt die Wahrheit irgendwo dazwischen? Tatsächlich legten die kassenpflichtigen Generika in der Schweiz 2006 erneut kräftig zu. Seit dem Jahr 2001 hat sich der Markt der Generika auf 381.2 Millionen Franken mehr
CHECKLIST & INFORMATION SHEET Catalina Adventurer Volunteer Payment – Cost for 2008 is $180. This price does not include boat transportation. Make checks payable to the Catalina Island Conservancy. Application – Complete application and mail to Santa Catalina Island Conservancy; Volunteer Services; PO Box 2739; Avalon, CA 90704


