
Cialis ist bekannt für seine lange Wirkdauer von bis zu 36 Stunden. Dadurch unterscheidet es sich deutlich von Viagra. Viele Schweizer vergleichen daher Preise und schauen nach Angeboten unter dem Begriff cialis generika schweiz, da Generika erschwinglicher sind.
Bjorl.org.br2
Documento descargado de http://bjorl.elsevier.es el 07/10/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
Rev Bras Otorrinolaringol
CASE REPORT
Rhinoscleroma: Case Report
Mônica Elisabeth Simons1, Lidio Granato2, Roberto
Claudio Batista Oliveira3, Mônica Porto Alves
Keywords: klebsiella rhinoscleromatis, microscopy,
Rhinoscleroma is a chronic, granulomatous infection that
most frequently affects the respiratory mucosa, especially the nasal cavity and eventually extending through the lower respiratory tract. The disease is endemic in some countries of Central America (El Salvador and Guatemala), Indonesia, India, Poland, Hungary, Russia and some African countries as well. It is a rare disease in South America. We report a 51-year-old male resident of a psychiatric institution in São Paulo presenting with progressive nasal obstruction, frontal headache, yellowish nasal discharge and a mass extruding through the right nasal vestibule. The present case report describes a Rhino-Sinus scleroma where histopathology was vital in the diagnosis. The patient was treated by surgical excision of the nasal mass followed by a course of ciprofloxacin. He has remained asymptomatic up to the last visit six months following treatment and has shown no evidence of recurrence.
1 MD, Otorhinolaryngology Intern - Santa Casa de São Paulo.
2 Assistant Professor - Department of Otrhinolaryngology - Santa Casa de Misericórdia de São Paulo.
3 MD, Otorhinolaryngologist.
4 MD, 3rd Year Resident - Santa Casa de Misericórdia de São Paulo.
Mailing Address: Mônica Elisabeth Simons - Rua Dom Constantino Barradas 88 apto. 42 São Paulo SP 04134-110.
Tel/Fax: (0xx11) 5062-6448 - E-mail:
[email protected]
Paper submitted to the ABORL-CCF SGP (Management Publications System) on March 7th, 2005 and accepted for publication on September 8th, 2005.
BRAZILIAN JOURNAL OF OTORHINOLARYNGOLOGY 72 (4) JULY/AUGUST 2006
http://www.rborl.org.br / e-mail:
[email protected]
Documento descargado de http://bjorl.elsevier.es el 07/10/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
limits. Psychiatrically the patient was confused and agitated due to mental deficiency.
Rhinoscleroma is a chronic granulomatous, slowly
Computed tomography of the paranasal sinuses
progressive infection that affects the nose and other res-
revealed a lesion with soft tissue attenuation material in
piratory tract structures1. It was first described in 1870 by
the nasal fossae, the right maxillary sinus, the anterior
the dermatologist Ferdinando Von Hebra2 and posteriorly
ethmoid cells, in some posterior ethmoid cells, and in
named respiratory scleroma. The Greek name "skleroma,"
part of the frontal sinus to the right. There was minor soft
meaning hard tumefaction, was adopted in 1932 at the
tissue attenuation material in the left maxillary sinus. The
International Clinical Otorhinolaryngology Conference (in
sphenoid sinus and the rhinopharynx were unaltered and
Madrid), emphasizing involvement of upper and lower
no bone destruction was observed. (Figures 1 and 2)
airways1,3. It occurs frequently in the nasal fossae, even-
Treatment included surgery followed by antibiotics.
tually extending itself to the larynx, the rhinopharynx, the
Surgical removal of the tumor from the nasal fossae was
mouth and the paranasal sinuses; the lips, trachea and
a sinusectomy through the transmaxillary approach with
bronchi may also be affected to a lesser degree4,5. Extra-
a degloving access route. The specimen was referred to
respiratory involvement has rarely been described1.
pathology for examination. At surgery a 3 cm diameter
Scleroma is endemic in some Central American
hard whitish-gray mass was found inserted in the right
countries (El Salvador and Republic of Guatemala), Indo-
maxillary sinus and the right nasal fossa, extending itself
nesia, India, Poland, Hungary, Russia and some African
into the ethmoid sinus; it had a smooth surface with irre-
countries1,6. In South America the frequency is low1,7.
gular contours and contained pus. Bone structures were
The first observation of scleroma published in Brazil
preserved and the cartilage septum was deviated to the
was made by Adolpho Lutz in 18908. Few cases have been
left by tumoral compression.
reported in Brazilian medical literature, thus the reason for
Pathology disclosed nasal mucosa containing a di-
publishing this case, which includes the histopathology
ffuse lymphoplasmacytic inflammatory process with large
and treatment.
vacuolated macrophages typical of Mikulicz cells and many plasmocytes transformed into Russel bodies. (Figure 3)
CLINICAL CASE PRESENTATION
Ciprofloxacin was used (500 mg. 12/12h for 14 days)
based on literature data.
J.P.S is a 51-year-old brown unmarried male patient
The patient returned to the Otorhinolaryngology
born in Minas Gerais, coming from Sao Paulo (SP state),
unit in good physical condition and no signs of recurrence
and living in a psychiatric support institution. He was
in the nasal mucosa.
brought to the Otorhinolaryngology unit at the Sao Paulo Santa Casa de Misericordia Hospital by his sister, and presented a reddish mass in his right nare, with frequent bleeding episodes, for the past five months. He also had a long history of sneezing, nasal pruritus, thickened and yellowish rhinorrhea, bilateral nasal obstruction, and daily intense frontal headaches.
On further investigation, he had lost some weight
(three kilograms) during those five months, and was an ex-smoker and ex-drinker of alcoholic beverages, having given up these habits four years ago. He had worked as a polisher, in contact with chemical products during 10 years, and had been retired due to a psychiatric condition (mental deficiency). He was taking biperiden, chlorpro-mazine and haloperidol, and lived in a psychiatric support institution.
The otorhinolaryngological exam revealed an enlar-
ged nose due to a violet-colored mass with small ulcers, a hardened consistency, a smooth surface, and irregular borders, which extruded from the right nare. The left nasal fossa was obstructed by a complete deviation of the nasal septum. It was not possible to introduce a nasopharyngos-
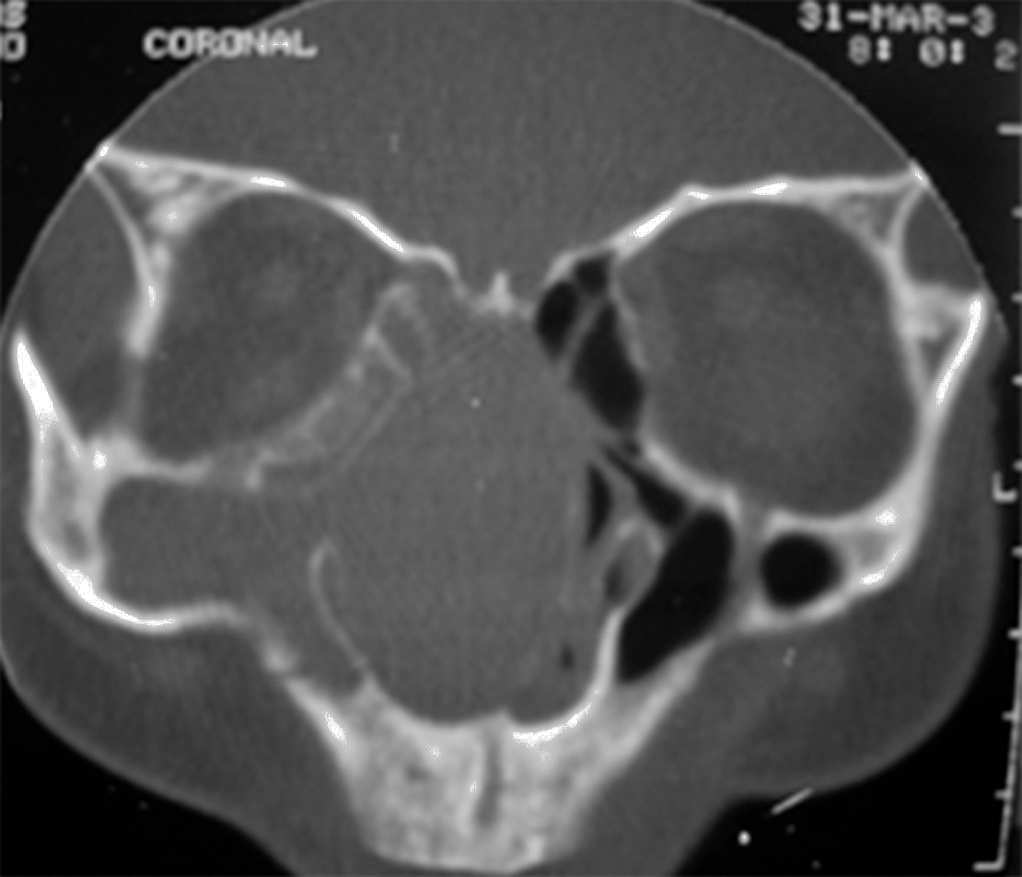
Figure 1. Computed tomography of the paranasal sinuses - coronal
cope. On examination with the Glatzel mirror, both nasal
plane. Soft tissue attenuation material occupies the nasal fossae, the
fossae were not pervious.
right maxil ary sinus, and some ethmoid cel s. The cartilaginous septum
The remaining physical exam was within normal
is deviated to the left. There is no bone destruction.
BRAZILIAN JOURNAL OF OTORHINOLARYNGOLOGY 72 (4) JULY/AUGUST 2006
http://www.rborl.org.br / e-mail: [email protected]

Documento descargado de http://bjorl.elsevier.es el 07/10/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
truction. This stage can last for weeks or months. (2) the hypertrophic stage: this stage includes granulation tissue with deformity by widening of the nasal pyramid, and nasal septum cartilage destruction. Epistaxis, anosmia, and anesthesia of the soft palate, among other symptoms, may occur. (3) the sclerotic stage: this stage is characterized by extensive scarring and laryngeal, and nasal vestibular stenosis in severe cases10,11.
Scleroma is an opportunistic disease in immunosup-
pressed patients and has many differential diagnoses, such as specific granulomatous diseases caused by bacteria (tu-berculosis, actinomycosis, syphilis and leprosy), by fungi (histoplasmosis, blastomicosis, paracoccidioidomycosis), by other parasites (mucocutaneous leishmaniasis), systemic diseases (sarcoidosis and Wegener's granulomatosis), and neoplasms (verrucous carcinoma)12.
The patient in our case had a tumor that extruded
from the right nare. It was typically a hypertrophic stage lesion. The first diagnosis, however, was of a neoplasm, al-though granulomatous diseases had not been excluded.
Given the emotional situation of the patient and
Figure 2. Computed tomography of the paranasal sinuses - axial plane.
based on the physical exam and radiographic data, we
Soft tissue at enuation material occupies the right nasal fossa, the right
decided for surgery even without a preoperative biopsy.
maxil ary sinus, and part of the left maxil ary sinus. The cartilaginous
The complete specimen was sent to pathology. Frequently
septum is deviated to the left. There is no bone destruction.
in these cases biopsies do not provide a final diagnosis, due to secondary contamination and insufficient material.
Histopathology defines the diagnosis based on fin-
ding Mikulicz cells and degenerated plasmocytes in Russel bodies, described in 1877 by Johann Von Mikulicz13. The etiological agent is Klebsiella rhinoscleromatis, a Gram-negative facultative intracellular encapsulated bacillus, a member of the Enterobacteriaceae family identified by Von Frisch in 188214.
Mikulicz cells are clear cytoplasm vacuolated his-
tiocytes containing the bacillus. Factors involved in trans-forming histiocytes into Mikulicz cells are unknown9.
Antibiotic treatment is used as a single treatment to
eradicate the infection mostly in the catarrhal stage, or as ancillary treatment in other stages of the disease to reduce mortality and avoid complications. Drug treatment may be combined with surgery in cases with granulomatous lesions
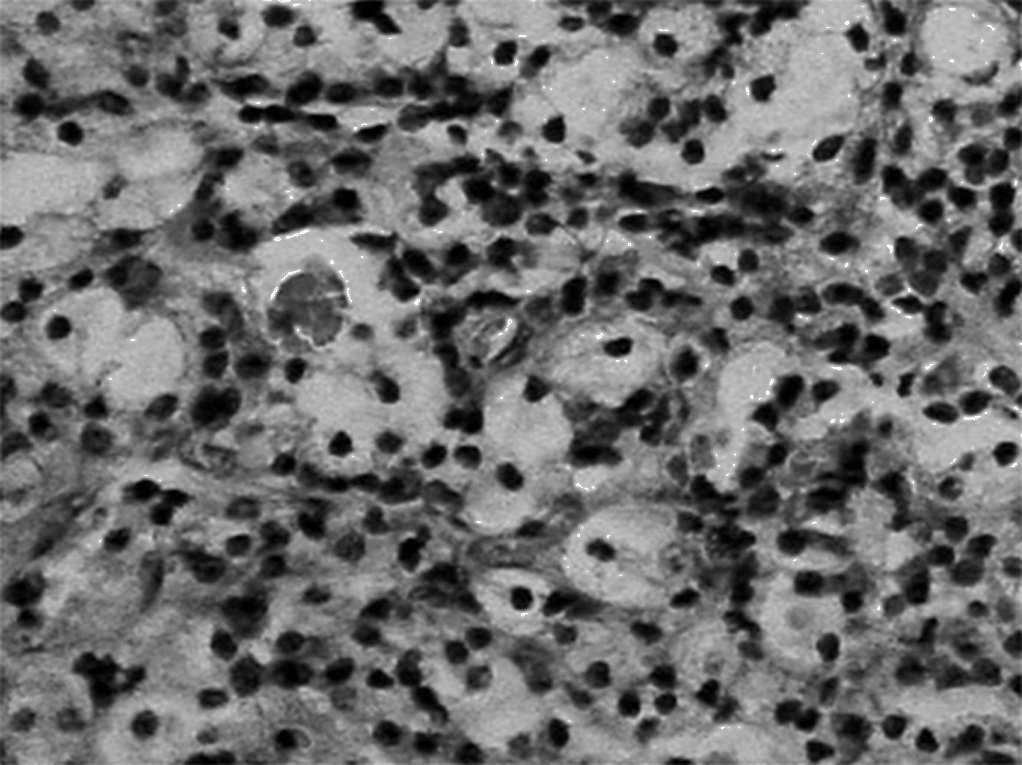
Figure 3. Microscopy exam of the nasal mucosa showing a lympho-
or scarring stenosis. Many antibiotics have been used to
plasmacytic infiltrate with Mikulicz cel s, Russel bodies and congested
treat rhinoscleroma. Streptomycin has severe side effects,
and dilated blood vessels.
especially on the vestibular system; also resistance to this drug has developed in a number of countries. Tetracycline
requires a prolonged course of treatment and also has sig-nificant adverse effects. Rifampicin provides good results
Scleroma is a specific granulomatous infection that
in the treatment of rhinoscleroma, but requires effective
affects the nose and, less frequently, other structures of
monitoring of toxicity. Trimethoprim-sulphamethoxazo-
the respiratory tract. It usually affects people with lower
le may be effective and is widely used in Third World
social and economic status, and is associated with lack of
countries. Recent studies have shown that the quinolones,
hygiene and prolonged contact with infected patients3,9.
ciprofloxacin and fluoroquinolone readily penetrate the
The disease progresses in three stages: (1) the ca-
tissues and are clinically effective3.
tarrhal stage: patients have non-specific rhinitis symptoms that progress to fetid rhinorrhea, crusting and nasal obs-
BRAZILIAN JOURNAL OF OTORHINOLARYNGOLOGY 72 (4) JULY/AUGUST 2006
http://www.rborl.org.br / e-mail: [email protected]
Documento descargado de http://bjorl.elsevier.es el 07/10/2016. Copia para uso personal, se prohíbe la transmisión de este documento por cualquier medio o formato.
Scleroma is a better name for this clinical entity,
1. Granato L, Jorge JJ, Souza DG, França LCM. Rinoscleroma - Conside-
as it affects both the nasal cavity and the remaining res-
rações sobre um caso. RBM - Otorrinolaringologia 1977;43(1):1-11.
2. Hebra FV. Vever ein eigent huemliches neugebilde ander nase. Wien
piratory tract. It is a rare condition in our country and
frequently is difficult to diagnose. This is due to the dise-
3. Badia L, Lund VJ. A case of rhinoscleroma treated with ciprofloxacin.
ase stages, where patients may present with non-specific
J Laryngology & Otology 2001;115:220-2.
rhinitis symptoms, signs of granulomatous proliferation
4. Wilson WR, Montgomery WW. Infectious diseases of the paranasal
sinuses. In: Paparella MM, Shumrick DA, Gluckman JL, Meyerhoff
or scarring.
WL, eds. Otolaryngology, III: Head and Neck. 3rd ed. Philadelphia:
When the disease progresses with proliferation, it
Saunders 1991; 1843-60.
may simulate a tumor, as in our patient. At a later stage,
5. Rifai M. Laryngotracheal resection for post scleromatous laryngeal
scarring may produce retraction in any part of the respi-
stenosis. J Laryngol Otol 1989;103:935-58.
6. Shaw HJ. Martin H. Rhinoscleroma. A clinical perspective. J Laryngol
ratory tract.
Otol 1961;1011-39.
Material should be adequate for histopathology.
7. Granato L, Mimica I, Mimica LMJ, et al. Rinoscleroma: apresentação
A cell infiltrate containing lymphocytes and plasmocytes
de um caso. Acta Awho 1985;4(2):47-50.
including Mikulicz cells and Russel bodies is highly sugges-
8. Lutz, A. Zur Kosmistik dês Rhinoskleroms, Monastsh F. prakt. Dermat
tive of scleroma. The differential diagnosis should be made
9. Kim NR, Han J, Kwon TY. Nasal rhinoscleroma in a nonendemic
with granulomatous diseases, leprosy and tuberculosis, all
area: a case report. J Korem Med Sci 2003;18:455-8.
of which may be identified with specific histopathological
10. Al Razek AKA, Al Elasfour A. MR appearance of rhinoscleroma: article.
Am J Neuroradiology 1999;20:575-8.
11. Becker TS, Shum TK, Waller TS, et al. Radiological aspects of rhinos-
Isolating Klebsilela Rhinoescleromatis using special
cleroma. Radiology 1981;141:433-8.
culture media is not always possible in these cases.
12. Al Serhani AM, Al Qahtani AS, Arafa M. Association of rhinoscleroma
The correct diagnosis is given based on histopatho-
with rhinosporidiosis. Rhinology 1998;36(1):43-5.
logical findings and the clinical history, which includes
13. Mikulicz J. Veber das rhinosclerom. Arch F Klin Chir 1877;20:485.
14. Von Frisch A. Zur aetiologie des rhinoskerons. Eien Méd Wschr
information on living conditions and the work environ-
BRAZILIAN JOURNAL OF OTORHINOLARYNGOLOGY 72 (4) JULY/AUGUST 2006
http://www.rborl.org.br / e-mail: [email protected]
Source: http://bjorl.org.br/en/pdf/S1808869415310065/S300/
This article was originally published in a journal published by Elsevier, and the attached copy is provided by Elsevier for the author's benefit and for the benefit of the author's institution, fornon-commercial research and educational use including without limitation use in instruction at your institution, sending it to specific
Important InformatIon on health and medIcal care IMPORTANT: If you are a citizen of the EU/EEA and can present a valid European health insurance card (EU-card) or are nationally registered in Sweden you are covered by the healthcare offered by the County Council of Västerbotten. You might also be covered by this healthcare if you are a non EU/EEA citizen. You must then have a residen-ce permit for more than a year and be nationally registered in Sweden. The


