
Cialis ist bekannt für seine lange Wirkdauer von bis zu 36 Stunden. Dadurch unterscheidet es sich deutlich von Viagra. Viele Schweizer vergleichen daher Preise und schauen nach Angeboten unter dem Begriff cialis generika schweiz, da Generika erschwinglicher sind.
GSTF International Journal of Psychology (JPsych) Vol.1 No.1, March 2014
The Cannabinoid-Memory and the Angiotensin-
Memory Paradoxes: Another Penrose Triangle?
Ramanujam N., MD,
Abstract— This study aims to evaluate the efficacy of two
different drugs in their effects on memory and discrimination
ngiotensin is a group of peptides consisting mainly of
learning in a dual, controlled mouse model of amnesia, and to
findings
Angiotensin I, Angiotensin II, Angiotensin III, and
pharmacodynamics profiles. It also aims at validating a sub-acute
Angiotensin IV. Each of these molecules can activate specific
scopolamine dose protocol as a model of rodent amnesia,
receptors for Angiotensin, named AT 1-4. Although each of
specifically of emotional memory.
these receptors has specific agonists and antagonists, they
The Exteroceptive models used include a Y-maze and an
could, in theory, be occupied by any of the above peptide
Elevated plus Maze (EPM). The Interoceptive models used are
two different dose protocols of an amnesic drug, Scopolamine in
Almost all the components of the Angiotensin system are
forty-eight Swiss Albino mice, categorized into an acute and a
sub-acute induction division, each of which later received fixed
found in the central nervous system. They regulate many
human equivalent doses of two drugs, apart from saline and
physiological and pathophysiological processes and are
scopolamine. Each animal was then evaluated for their Novelty
responsible for maintaining vital functions, ranging from blood
Object Recognition (NOR) memory, and visuo-spatial memory,
pressure regulation to sexual function. Perhaps the most
on the Y-maze and the EPM, respectively. The results of the
important of these functions relevant to the current study is
Novelty Preference Test (NPT) and EPM test were analysed using
memory and its regulation and modulation.1
Analysis of Variance.
The efficacy of Rimonabant in improving NOR memory was
Similar to this system in its central role, is the
statistically higher than in saline and model control groups, more
endocannabinoid system. This system consists of two well
so in the acute induction. Its efficacy in enhancing visuo-spatial
characterized (CB1, CB2) and one poorly characterized
memory was less, although comparable to that on NOR memory.
receptor (Anandamide Receptor).2 The endocannabinoids are a
The efficacy of Valsartan was lower than the NOR Recognition
group of lipid-derived compounds including Anandamide
Indices of other groups, although insignificant statistically. Sub-
acute induction resulted in increased amnesia and anxiety in the
Valsartan group on both mazes, the former being comparable to
Tetrahydrocannabinol, and 2-Arachidonyl derivatives.
that noted in scopolamine group.
Cannabinoids mediate dopamine induced increase in reward
Rimonabant is a memory enhancer, in terms of both
behaviour through activation of CB1 receptors in nucleus
recognition and spatial memory. Valsartan is a pro-amnesic drug
accumbens.3 Rimonabant could act through this pathway in the
in a sub-acute induction, in which it lead to increased anxiety
brain to increase acquisition of reward memory induced by
additionally. Hence, sub acute scopolamine protocol could be a
psychostimulants like cocaine. Moreover, disrupting CB1
novel model of emotional memory. Though many drawbacks were
noted in the study, the drug effects could be explained by
signalling by knocking out CB1 gene and then treating the
pharmacokinetic data and pharmacodynamic effects. This pilot
mice with Rimonabant repeatedly impairs spatial memory
study could be used for correlating the results in human
extinction on Morris water maze.4 There is also evidence that
conditions involving memory.
endocannabinoids affect inhibitory avoidance learning, but
their effects on working long term memory lack proper
Index Terms— Cannabinoid Receptor, Angiotensin Receptor,
Rimonabant, Valsartan, acute Scopolamine amnesia, maze
learning, novelty object recognition memory, spatial memory, sub-
On similar lines of reference, Angiotensin system through
acute scopolamine amnesia, y-maze, elevated plus maze
AT4 receptors and AT1-containing neurons in areas of brain, mediate memory and learning.6 Angiotensin IV-mediated
antagonism of hippocampal neurotransmission using an AT4-
Manuscript received November 17, 2013. This work was entirely done at
CEFT, Sri Ramachandra University, Chennai, and the author wishes to
specific antagonist attenuates acetylcholine release.7 It has
acknowledge Parvathavarthini S., MD, and Seethalakshmi S., MD, for their
already been an established fact8 that increases in hippocampal
research and academic guide ships, knowledge base, and conceptual support.
acetylcholine improves memory and even prevents memory
The work was self-funded by the author, as a part of MD dissertation. The author acknowledges Sigma Aldrich India for the timely supply of
decline due to deposition of insoluble beta amyloid in brain.9,10
Hence, we tried to evaluate whether or not Rimonabant and
Ramanujam N. is with the Department of Pharmacology of PSG Institute
valsartan, acting through distinct mechanisms, improve
of Medical Sciences & Research, Coimbatore - 641004, India (phone +91-
working long term memory and spatial-emotional memory.
9790532350; e-mail.
This study aims to evaluate the acute and sub-acute
DOI: 10.5176/0000-0002_1.1.5
GSTF International Journal of Psychology (JPsych) Vol.1 No.1, March 2014
efficacies of Rimonabant and Valsartan in improving cognition in scopolamine mouse model of amnesia.
The hypothesis was that administering each drug to different
anticholinergic, scopolamine, could lead to memory changes related, in some way, to the cholinergic system.
II. MATERIALS & METHODS
A. Ethical & Regulatory Considerations:
The study was accepted and permitted ethically by the
Institutional Animal Ethics Committee (IAEC Approval Number: SRU/CEFT/LE/016/111/2009, dated 06 August
2009), and was conducted in a laboratory-cum-animal facility
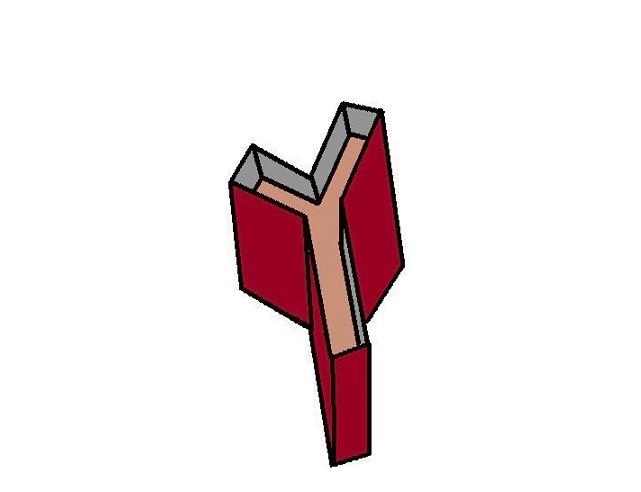
FIGURE 2: Y-maze: Note the two arms, novel and start
(SRU-CEFT) following Committee for the Purpose of Control
arms are of equal lengths; the third longer arm is the
& Supervision of Experiments on Animals (CPCSEA) and
familiar arm (not shown: the guillotine door in the
Good Laboratory Practices (GLP) guidelines.
central platform, adjacent novel arm opening).
B. Materials:
The study drugs: Rimonabant is a Cannabinoid receptor
Scopolamine was purchased from Sigma-Aldrich, India, and
partial antagonist that was initially approved for treatment of
the study drugs Valsartan and Rimonabant were purchased
obesity as an anorectic drug and later retracted due to high
from local manufacturers. Mazes used for this study were of
incidence of suicidal tendencies. Valsartan is an Angiotensin
the standard dimensions:
receptor antagonist that is also used clinically as
antihypertensive drug. Both were given separately to two
different groups by oral gavage. Rimonabant was given as a
Y-maze: 75 cm × 16 cm × 35 cm,
3% solution in water, whilst valsartan as a 10% aqueous
* Dimensions of each maze = length (total) × breadth (total)
× height (total). The following figures (Figs. 1 & 2) depict the
Controls: Saline 0.5% was used to serve as non-vehicle
design of these mazes used in this study.
non-treatment control for the first group. Scopolamine 3% in water served as the memory decline control for the acute study, whereas scopolamine 0.5% in water served as the amnesia control for the sub-chronic study. The study design and duration did not warrant the need for ageing control to remove ageing-related amnesia as a confounder.
Saline and scopolamine were both given by intra-peritoneal
route. Scopolamine was injected also in the two test groups, prior to drug treatments.
Animals & grouping: Forty eight Swiss albino mice were
obtained and grouped into two divisions – acute and sub-acute amnesia induction divisions. Under each division, four equally
numbered groups were obtained randomly as per body weight
FIGURE 1: Mouse Elevated plus Maze; Note the
using a table of random numbers.
enclosed arms have thicker walls (in white shade) and
Exteroceptive models: A study plan using a y-maze
open arms have no walls (shown here as having a thin
protocol was used to evaluate the working and novelty
layer of single wall)
preference long term memory. On similar lines of reference, an
elevated plus maze protocol was used to evaluate the spatial
long term memory. Both forms of memory were not evaluated using the test drugs before. Both mazes were also used to study other possible effects like those on anxiety, behaviour, and motor activities.
Interoceptive models: Scopolamine was used to induce
amnesia as a single high dose (acute amnesia) and as multiple daily once low doses for seven days (sub-acute amnesia). As it disrupts muscarinic system-mediated cholinergic transmission, it was the best Interoceptive model for the present study.
GSTF International Journal of Psychology (JPsych) Vol.1 No.1, March 2014
The following diagram depicts the animal grouping,
treatment and evaluation plans (Fig. 3):
Where, R.I. = Recognition Index, NAE = Number of Arm Entries, N & F = Novel & Familiar arms. EPM: The transfer latency (T.L.) test was used to assess the
spatial memory that was fear-related. The maze consisted of four arms of equal dimensions at ninety degrees orientation to each other in the horizontal plane, elevated from the floor. The two opposite pairs of arms differed from each other, in that one pair was open (no walls), the other one enclosed (surrounded by walls on all three sides, except that facing the central platform). In this test, in a single trial each in the two divisions, the mouse was placed in the central platform, that it faced one of the open arms. The upper cut-off time was 90
Seconds, above which if the mouse did not move into either
of the enclosed arms, three fourths of its body length inside the arm, it was discarded from the study. The endpoint was transfer latency, the time taken by it to move from its starting initial position in the maze to this enclosed arm, is a direct measure of its Nootropic effect, inversely its anxiogenic effect.
Scopolamine Treatments: Scopolamine is an anticholinergic
drug used as a transdermal therapeutic system in patients with
FIGURE 3: Study Grouping and Treatment-Evaluation
motion sickness. It is also an amnestic agent, when injected in
In the acute amnesia induction, it is injected by
intraperitoneal route as a single high dose of 3 mg/kg in
C. Methodology:
mouse. This was followed by single oral drug treatments.
Each division was assessed for the parameters using
For the sub acute induction, it can be injected in multiple
separate animals.
low doses on a daily basis for 7, 14, 21 days. In the present
study, it was used as a daily 0.3-0.5 mg/kg injection for seven
Y-Maze: The novelty preference test (NPT) was used to
days, followed by drug treatments for an another three days.
assess the working long term memory and novelty memory on
y-maze after acute and sub-acute scopolamine treatment. In this test, the asymmetrical y-maze was used (refer figure 2), in
D. Statistical Analyses:
which two arms were of equal dimensions, the third being
Single factor analysis of variance (ANOVA) was used to
longer in length. One of the equal arms had a guillotine door
compare all the parameters in each group, followed by
near its junction with the central platform, where all three arms
appropriate post-hoc tests like Tukey test or Bonferroni-Holm
test. Statistical significance was kept at less than five percent.
This door was designed in a manner so as to allow opening
or closing of this arm, as and when required. This arm
All tests were performed using MS-excel 2010 and Daniel
equipped with the door was the novel (N) arm; the other
XL-toolbar, a statistical add-in for MS-excel.
equivalent adjacent arm was the start (S) arm; the longer arm
was the familiar (F) arm. The familiar arm was longer so as to neutralize the confounding effects of initial exploratory trials
in its longer length, relative to the novel arm which was closed
in these trials.
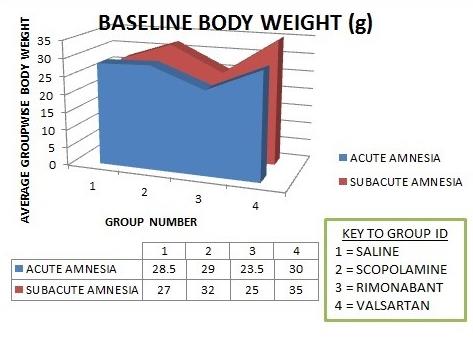
A. Baseline characteristics:
The recognition index (R.I.) was used in later acquisition
The body weight of all the animals used fell in the 23-36 g
trials (one hour, two hour, four hour, and twenty four hours,
range at the baseline. They were then randomized based on
post last drug treatment). It is a measure of novelty preference
these weights into two divisions, presumably weighed equally
working long term memory, based in the hippocampal
group-wise. The numbers of male and female mice in each
pathways. It is calculated using the formula:
division were comparable.
GSTF International Journal of Psychology (JPsych) Vol.1 No.1, March 2014
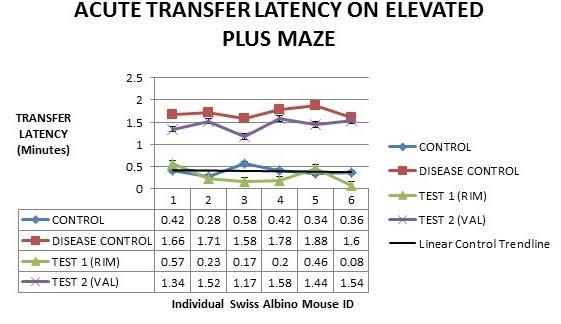
differences in the transfer latencies between all two-group
comparisons except that between Rimonabant group and saline control group ( p = 0.14).
This would mean that the Rimonabant group did not differ
significantly in its Nootropic efficacy as the saline control group. Additionally the Valsartan group was comparable to the scopolamine group in its pro-amnestic efficacy in a statistically significant manner (p = 0.001). The following figure (Fig. 6) summarizes these results:
FIGURE 4: Baseline Body Weight Characteristics
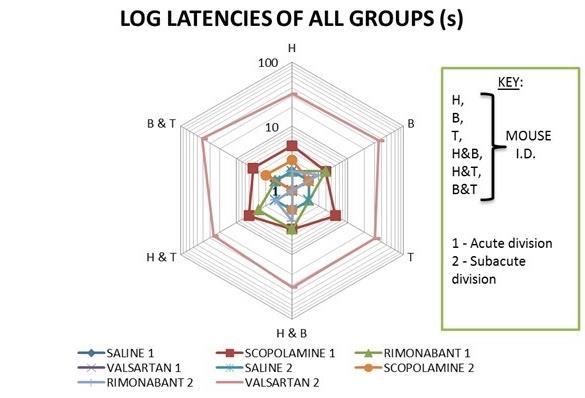
B. Y-maze: latency to locomotion: Post analysis of variance of the data depicted in figure 5,
one can deduce that the comparison of sub-acute induction
valsartan group was significantly different from the latencies in
all other groups, although equal variances could not be
FIGURE 6: Depicts line plot of transfer latencies
assumed (p < 0.05). From figure 5, one can infer the above
(seconds) of all four groups in acute amnesia division.
result since, it is that only group latency that is deviating from
the normal value (since rodents are exploratory, latency will
normally expected to be zero seconds).
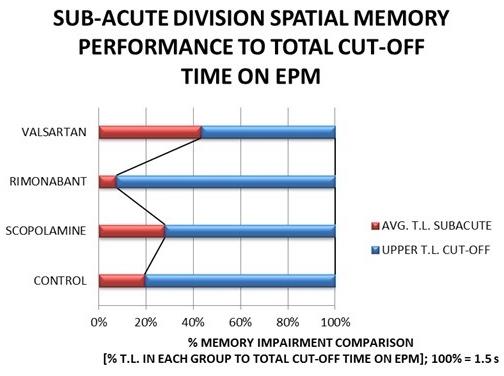
D. Sub-acute division: elevated plus maze:
In this test, one can appreciate from figure 7, that valsartan
group is comparable to scopolamine group in its spatial memory disruption, compared to the other two groups. Note that 100% impairment refers to the condition when transfer latency approaches cut-off time of one and a half minutes.
FIGURE 5: Shows semi-logarithmic plots of latencies to locomotion (seconds) of all groups in each division (centripetal axis) against individual mouse ID (circumferential axis)
C. Acute division: elevated plus maze:
The acute scopolamine induction in mice and the
Performance on EPM with the Trial Cut-Off as
subsequent testing of spatial memory on the elevated plus
100%; Sub-Acute Avg. T.L.
maze showed statistically significant intergroup comparison
GSTF International Journal of Psychology (JPsych) Vol.1 No.1, March 2014
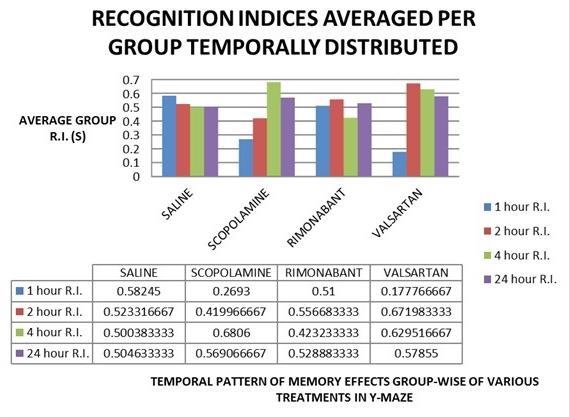
E. Y-maze: recognition indices: Though the basic assumptions for ANOVA were met with
reference to the y maze NPT, and further, an insignificant comparison (p>0.05), the results are important in explaining the temporal actions of the treatments on memory (Refer Figure 8 and discussion, later).
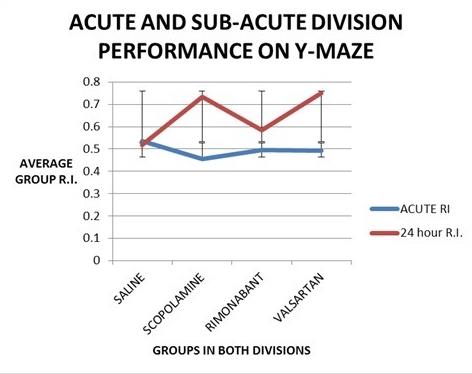
Figure 9: GroupWise Trend Lines for Y-Maze NPT Performances in Acute & Sub acute Amnesia (Error
Bars Denote Avg. R.I. ± S.E.M.)
B. EPM Results: From figures 6 & 7, one can conclude the similarly
efficacious detrimental effects of both valsartan and
scopolamine groups on spatial fear-related memory acutely
FIGURE 8: Group-Wise Temporal Y-Maze Novelty
and sub acutely. There was some improvement with
Recognition Indexes Pattern
Rimonabant treatment with spatial memory acutely. Of notable
is that the valsartan showed increased anxiety on open arms on
the EPM, as shown by transfer latencies approaching the cut-off times in the sub-acute amnesia model, and increased
rearing on the open arms.
A. Y-maze Results:
As notable form figure 9, the memory improvement was
C. Extrapolation of the results to human beings:
stable among the four groups in the acute amnesia model more
The results could be extrapolated readily to human disorders
than in the 24 hour trial. There tends to be better intergroup
like vascular and degenerative dementias. Rimonabant is
comparison in sub acute than in acute division, and a better
moderately nootropic in acute dementia where spatial memory
improvement in working memory in 24 hour trial than in acute
is disrupted, like delirium and Korsakoff Wernicke's psychosis
amnesia trials. Even in the sub acute division, performance
and acute epileptic syndromes involving temporal lobes.
was better in scopolamine and valsartan groups, as a paradox.
Valsartan may be effective more in vascular than degenerative
Finally, Rimonabant group was borderline (0.6%) in its
dementias like lewy-body and Alzheimer's' type; it may even
memory effects in sub acute division. The paradoxical effects
cause working memory disruption in the latter types of
could be partially explained by U-shaped dose response
relationship that is inherent of most of the toxicological
compounds like scopolamine.11,12,13,14 Valsartan could follow
D. Pharmacodynamic & pharmacokinetic considerations:
similar effect relationship the peaks might be mediated by AT1
Evidence also indicates the presence of interactive synaptic
and later by AT4 receptors, the trough by AT2 receptors,
pathways and neural networks underlying the intertwined
owing probably to differential affinities of valsartan to these
communicative neuroeffectors that could partly explain the
drugs' effects observed in this study. 15 Indeed such
Rimonabant did show borderline memory improvement
interactions are now known to mediate key physiological
which may be due to its multiple dosing which did not have the
processes, including those of cannabinoid, and, gastrointestinal
efficacy in modulating dopaminergic system transmission
with neurokininergic, 16 and cognitive and addictive behavior
through CB1 receptors, and due to its unfavorable
with glutaminergic and GABAergic pathways. 17 In contrast to
pharmacokinetics on repeated dosing.
Cannabinoid system, direct stimulation of cognitive processes
by Angiotensin II 18 and Angiotensin IV 19, 20 ligands have been
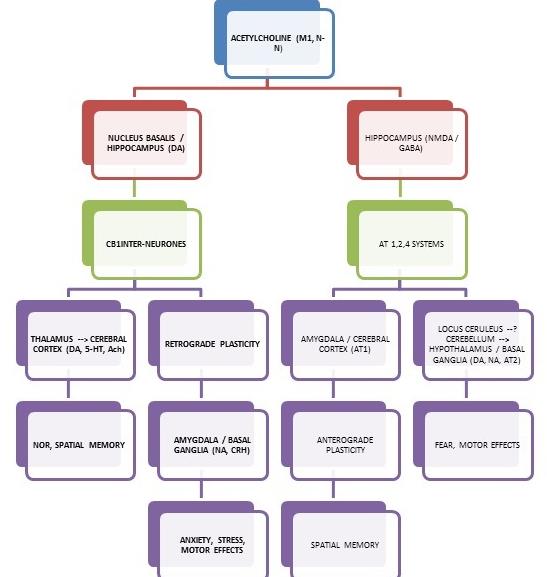
known, in-spite of controversial 21, 22, 23, 24 26 mechanisms. Interfacing such results with the accepted mechanisms of
GSTF International Journal of Psychology (JPsych) Vol.1 No.1, March 2014
memory processes evaluated in this study, and, using the
results of this study, a working model could be developed for the memory actions of both study drugs, as follows (figure 10 & 11):
FIGURE 11: TIME-LINE OF ACTION OF THE
STUDY DRUGS AND AMNESIC INDUCER ON
TOGETHER (Figure not to scale)
The above figure (Fig. 11) states no more than that
pharmacokinetic parameters must be carefully prioritized a-priori in planning such multi-drug-efficacy evaluations.
E. Drawbacks: Although the study lacks statistical power and a
considerable effect size, it must be considered as a pilot study, and encourage the evaluation of these drugs on memory both preclinically and clinically, since, Rimonabant could even
reverse memory loss as a novel drug, whilst valsartan could be
disrupting memory in hypertensive patients on this medication.
Infact Rimonabant is known for its pleotropic effects in human
FIGURE 10: A WORKING MODEL TO EXPLAIN
THE PHARMACODYMAMIC EFFECTS OF THE
Biochemical parameters could not be evaluated herein due
TWO DRUGS USED IN THIS STUDY (NOR =
to financial constraints on the author.
Novelty object recognition memory), M1, N-N, AT1-
4 = Neurotransmitter receptors, DA, GABA, NMDA,
F. Conclusion:
5-HT, Ach = Neurotransmitters, CRH = Hormonal
Both cannabinoid and angiotensin systems could play
critical roles in cognition and behaviour, that could commonly
be related to cholinergic system. The study must be definitely
As the figure above (Fig. 10) clearly indicates, the three
followed up by further evaluations, aiming to explain the
paradoxes in this study.
Scopolamine model), Cannabinoid (represents Rimonabant's
Other forms of memory and cognitive processes must also
action), and Peptidergic (Angiotensin system represents
be considered in the use of both the study drugs for further
Valsartan's mode of action) systems are intertwined in brain
research and in clinical practice. Indeed this area of cognitive
areas to display possibly the phenotypic results observed in
psychology remains unexplored, though it may be yet another
impossible illusion much like the Penrose triangle.
The pharmacokinetic surrogate endpoints involved have not
been summarized previously elsewhere as a timeline. Scopolamine follows "hormesis" dose-response curves (U-shaped in contrast to bell shaped) owing to its toxic mechanism on cholinergic system14 in causing amnesia over its four-five half-live period. Note the dual-shaped nootropic-amnesic action of Valsartan, and bimodal action of Rimonabant as a nootropic agent, over each of their four-five half-lives, when the body concentration stabilize for such drugs.
GSTF International Journal of Psychology (JPsych) Vol.1 No.1, March 2014
7) Jing F, Mogi M, Sakata A, Iwanami J, Tsukuda K, Ohshima K, Min LJ, Steckelings UM, Unger T, Dahlöf B, Horiuchi M. (2012) Direct stimulation of angiotensin II type 2 receptor enhances spatial memory. J Cereb Blood Flow Metab. 32(2):248-55.
8) Wright JW, Harding JW. (2011) Brain renin-angiotensin--a new look at an old system. Prog Neurobiol. 95(1):49-67.
9) Benoist CC, Wright JW, Zhu M, Appleyard SM, Wayman GA, Harding JW. (2011) Facilitation of hippocampal synaptogenesis and spatial memory by C-terminal truncated Nle1-angiotensin IV analogs J Pharmacol Exp Ther. 339(1):35-44.
10) Pederson ES, Krishnan R, Harding JW, Wright JW. (2001) A role for
the angiotensin AT4 receptor subtype in overcoming scopolamine-induced
spatial memory deficits. Regul Pept. 102(2-3):147-56.
FIGURE 12: The Impossible Penrose Triangle
Wang J, Ho L, Chen L (2007) Valsartan lowers brain β-amyloid protein
levels and improves spatial learning in a mouse model of Alzheimer disease. J
Illusion: The Cannabinoid-Angiotensin-Cholinergic
Clin Invest. 117: 3393-402.
interactions – how many such inexplicable areas
are still hidden in cognitive psychology?
12) Ostrovskaya RU, Firova FA, Trofimov SS. (1995) Sustained Aftereffect
of the Amnestic Action of Scopolamine in Rats and Its Elimination by
Piracetam. Exp Biol. 359-61.
13) Quartermain D, Leo P. (1988) Strength of Scopolamine-Induced Amnesia as a Function of Time between Training and Testing. Behav and
Neural Biol. 300-10.
The author of the research entitled "THE CANNABINOID-
14) Agrawal R, Tyagi E, Saxena G, Nath C. (2009) Cholinergic influence on
MEMORY & THE ANGIOTENSIN-MEMORY PARADOXES:
memory stages: A study on scopolamine amnesic mice. Ind J Pharmacol.
ANOTHER PENROSE TRIANGLE?" endorses the originality
of the research, to his best professional competency. This
original research of the aforesaid author was entirely carried
15) Ledent C, Valverde O, Maldonado R, Bura SA, Castan A. (2007) Genetic and pharmacological approaches to evaluate the interaction between
out at CEFT, Sri Ramachandra Medical College & Research
the cannabinoid and cholinergic systems in cognitive processes. Br J
Institute, Chennai.
Pharmacol. 758-65.
16) Anonymous, Cannabinoids and the Gastrointestinal tract, Gut 2001;
48:859–867
17) Fernando Rodríguez De Fonseca, Ignacio Del Arco, Francisco Javier Bermudez-Silva,Ainhoa Bilbao, Andrea Cippitelli et Miguel Navarro, The
1) Yu LL, Zhou SJ, Wang XY, Liu JF, Xue YX, Jiang W, Lu L. (2011)
Endocannabinoid system: Physiology and Pharmacology, Alcohol &
Effects of cannabinoid CB₁ receptor antagonist Rimonabant on acquisition
Alcoholism 2004 Page 1 of 13, doi:10.1093/alcalc/agh110, available online at
and reinstatement of psychostimulant reward memory in mice. Behav Brain
Res. 217(1):111-6.
18) Fei Jing, Masaki Mogi, Akiko Sakata, Jun Iwanami, Kana Tsukuda,
2) Abush H, Akirav I. (2010) Cannabinoids modulate hippocampal memory
Kousei Ohshima, et al., Direct stimulation of angiotensin II type 2 receptor
and plasticity. Hippocampus. 20 (10):1126-38.
enhances spatial memory, Journal of Cerebral Blood Flow & Metabolism
(2012) 32, 248–255.
3) Yu LL, Wang XY, Zhao M, Liu Y, Li YQ, Li FQ, Wang X, Xue YX, Lu
L. (2009) Effects of cannabinoid CB1 receptor antagonist Rimonabant in
19) Eric S. Pederson, Radika Krishnan, Joseph W. Harding, John W.
consolidation and reconsolidation of methamphetamine reward memory in
Wright, A role for the angiotensin AT receptor subtype in overcoming
mice. Psychopharmacology (Berl).204(2):203-11.
scopolamine-induced spatial memory deficits, Regulatory Peptides 102
Ž2001. 147–156.
4) Robinson L, McKillop-Smith S, Ross NL, Pertwee RG, Hampson RE,
Platt B, Riedel G . (2008) Hippocampal endocannabinoids inhibit spatial
20) Caroline C. Benoist, John W. Wright, Mingyan Zhu, Suzanne M.
learning and limit spatial memory in rats. Psychopharmacology (Berl).
Appleyard, Gary A. Wayman, and Joseph W. Harding, Facilitation of
Hippocampal Synaptogenesis and Spatial Memory by C-Terminal Truncated
5) Varvel SA, Anum EA, Lichtman AH. (2005) Disruption of CB (1)
receptor signalling impairs extinction of spatial memory in mice.
Psychopharmacology (Berl).179(4):863-72.
21) John W. Wright, Joseph W. Harding, The brain angiotensin system and
6) Tota S, Hanif K, Kamat PK, Najmi AK, Nath C. (2012) Role of central
extracellular matrix molecules in neural plasticity, learning, and memory,
angiotensin receptors in scopolamine-induced impairment in memory,
Progress in Neurobiology 72 (2004) 263–293.
cerebral blood flow, and cholinergic function. Psychopharmacology (Berl).
22) S.Indumathy, S.Kavimani, K.V.Raman, Role of Angiotensin Antagonists in Memory Enhancement, International Journal of Pharma and Bio Sciences, Vol.1/Issue-3/Jul-Sep.2010.
GSTF International Journal of Psychology (JPsych) Vol.1 No.1, March 2014
23) Paul R Gard, Cognitive-enhancing effects of angiotensin IV, BMC Neuroscience 2008, 9(Suppl 2):S15 doi: 10.1186/1471-2202-9-S2-S15.
24) Laura E Wise, Philip A Iredale, Rene J Stokes, Aron H Lichtman, Combination of Rimonabant and Donepezil Prolongs Spatial Memory Duration, Neuropsychopharmacology (2007) 32, 1805–1812.
25) Maurizio Bifulco, Claudia Grimaldi, Patrizia Gazzerro, Simona Pisanti, Antonietta Santoro, Rimonabant: Just an Antiobesity Drug? Current Evidence on Its Pleiotropic Effects, Mol Pharmacol 71:1445–1456, 2007.
26) G. Riedel, · S.N.Davies, Cannabinoid Function in Learning, Memory and Plasticity, HEP (2005) 168:445–477, Springer-Verlag.
Dr. Ramanujam received his bachelors' degrees in Medicine and
Surgery (MBBS) from Sri Ramachandra University (Chennai, India)
in 2008. He received his postgraduate degree in medicine in 2011
with Pharmacology as the specialty (MD). He holds a fellowship in
clinical research from Medvarsity and Apollo Hospitals (Hyderabad,
India), and is a member of Indian Pharmacological Society, and
formerly of the Drug Information Association. He is currently
working as Assistant Professor in Pharmacology at PSG IMS&R,
Coimbatore, India, and is involved in academics and biomedical
research.
Dr. Ramanujam is interested in planning and execution of phenotypic
and proteomic / genetic / epigenetic studies involving pre-clinical and
clinical psychopharmacology, and cardiovascular pharmacology. He
is currently involved in pursuing his doctorate in Philosophy (Ph.D.)
in cognitive neurotoxicology. He holds one indexed, peer reviewed
International journal publication, and two indexed International peer
reviewed Conference Proceedings.
He was in the Technical Program Committee (TPC) of International
Conference on Cognitive & Behavioral Psychology (CBP) from 2011
through 2014, and is currently in the TPC of CBP 2015, and also is
an associate editor of GSTF Journal of Psychology. He was a member
of panel discussion in CBP 2011, held at Singapore. He is also co-
authoring a book entitled, "Target: Cognition," as the chief editor,
which is all about the established and prospective drugs and agents
targeting the higher cognitive functions with special emphasis on
drug discovery, development, and regulation.
Source: http://dl6.globalstf.org/index.php/jpsych/article/download/116/113
AGENZIA INTERNAZIONALE PER LA PREVENZIONE DELLA CECITÀSEZIONE ITALIANA Oftalmologia Sociale – Rivista di Sanità Pubblica Capo Redattoredott. Filippo CRUCIANI Comitato di redazioneprof. Luciano CERULLIdott.ssa Cristina MARTINOLIprof. Ugo MENCHINIprof. Giovanni SCORCIA COMITATO SCIENTIFICO NAZIONALE
European Journal of Echocardiography (2009) 10, 194–212doi:10.1093/ejechocard/jep005 EAE RECOMMENDATIONS Contrast echocardiography: evidence-basedrecommendations by European Associationof Echocardiography Roxy Senior1*, Harald Becher2, Mark Monaghan3, Luciano Agati4, Jose Zamorano5,Jean Louis Vanoverschelde6, and Petros Nihoyannopoulos7 1Department of Cardiology, Northwick Park Hospital, Imperial College, London, Harrow HA1 3UJ, UK; 2John RadcliffeHospital, Oxford, UK; 3King's College Hospital, London, UK; 4La Sapienza University, Rome, Italy; 5Hospital Clı´nico San Carlos,Madrid, Spain; 6Cliniques Universitaires St-Luc, Universite


