
Cialis ist bekannt für seine lange Wirkdauer von bis zu 36 Stunden. Dadurch unterscheidet es sich deutlich von Viagra. Viele Schweizer vergleichen daher Preise und schauen nach Angeboten unter dem Begriff cialis generika schweiz, da Generika erschwinglicher sind.
Pntd.0002605 1.10
Scrub Typhus Is an Under-recognized Cause of AcuteFebrile Illness with Acute Kidney Injury in India
Vivek Kumar1, Vinod Kumar1, Ashok K. Yadav1, Sreenivasa Iyengar1, Ashish Bhalla2, Navneet Sharma2,
Ritesh Aggarwal3, Sanjay Jain2, Vivekanand Jha1,4*
1 Departments of Nephrology, Postgraduate Institute of Medical Education and Research, Chandigarh, India, 2 Internal Medicine, Postgraduate Institute of Medical
Education and Research, Chandigarh, India, 3 Pulmonary and Critical Care Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, India,
4 George Institute for Global Health, New Delhi, India
Background: Infection-related acute kidney injury (AKI) is an important preventable cause of morbidity and mortality in thetropical region. The prevalence and outcome of kidney involvement, especially AKI, in scrub typhus is not known. Weinvestigated all patients with undiagnosed fever and multisystem involvement for scrub typhus and present the pattern ofrenal involvement seen.
Methods: From September 2011 to November 2012, blood samples of all the patients with unexplained acute febrile illnessand/or varying organ involvement were evaluated for evidence of scrub typhus. A confirmed case of scrub typhus wasdefined as one with detectable Orientia tsutsugamushi deoxyribonucleic acid (DNA) in patient's blood sample by nestedpolymerase chain reaction (PCR) targeting the gene encoding 56-kDa antigen and without any alternative etiologicaldiagnosis. Renal involvement was defined by demonstration of abnormal urinalysis and/or reduced glomerular filtrationrate. AKI was defined as per Kidney Disease: Improving Global Outcomes (KDIGO) definition.
Results: Out of 201 patients tested during this period, 49 were positive by nested PCR for scrub typhus. Mean age of studypopulation was 34.1614.4 (range 11–65) years. Majority were males and a seasonal trend was evident with most casesfollowing the rainy season. Overall, renal abnormalities were seen in 82% patients, 53% of patients had AKI (stage 1, 2 and 3in 10%, 8% and 35%, respectively). The urinalysis was abnormal in 61%, with dipstick positive albuminuria (55%) andmicroscopic hematuria (16%) being most common. Acute respiratory distress syndrome (ARDS) and shock were seen in 57%and 16% of patients, respectively. Hyperbilirubinemia was associated with AKI (p = 0.013). A total of 8 patients (includingthree with dialysis dependent AKI) expired whereas rest all made uneventful recovery. Jaundice, oliguria, ARDS and AKI wereassociated with mortality. However, after multivariate analysis, only oliguric AKI remained a significant predictor of mortality(p = 0.002).
Conclusions: Scrub typhus was diagnosed in 24% of patients presenting with unexplained febrile illness according to astrict case definition not previously used in this region. Renal abnormalities were seen in almost 82% of all patients withevidence of AKI in 53%. Our finding is contrary to current perception that scrub typhus rarely causes renal dysfunction. Wesuggest that all patients with unexplained febrile illness be investigated for scrub typhus and AKI looked for in scrub typhuspatients.
Citation: Kumar V, Kumar V, Yadav AK, Iyengar S, Bhalla A, et al. (2014) Scrub Typhus Is an Under-recognized Cause of Acute Febrile Illness with Acute KidneyInjury in India. PLoS Negl Trop Dis 8(1): e2605. doi:10.1371/journal.pntd.0002605
Editor: Nicholas P. Day, Mahidol University, Thailand
Received July 24, 2013; Accepted November 10, 2013; Published January 30, 2014
Copyright: ß 2014 Kumar et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permitsunrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: VJ has funding from the Department of Biotechnology and the Indian Council of Medical Research. The funders had no role in study design, datacollection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
* E-mail:
[email protected]
Pacific region with a case fatality rate of up to 30% in untreatedcases and stresses the need for its surveillance [1]. Scrub typhus has
Infections are responsible for a substantial portion of commu-
been reported from various parts of India [3–8], and has recently
nity acquired acute kidney injury (AKI) in India. The commonly
been identified as one of the important neglected zoonoses of
implicated conditions include malaria, leptospirosis, dengue,
public health importance [9].
enteric fever, viral and bacterial infections. Despite being endemic
Scrub typhus is considered as an uncommon cause of AKI
in Asia with an estimated one million cases occurring annually,
even in endemic areas. Renal involvement is thought to be a
scrub typhus, caused by the rickettsia Orientia tsutsugamushi, is highly
consequence of multi-organ dysfunction syndrome secondary to
underdiagnosed and under-reported cause of hospitalization [1,2].
sepsis [10,11]. In part, this has been due to inability to make an
World Health Organization (WHO) identifies scrub typhus as a
accurate diagnosis due to non-availability of investigations. Recent
re-emerging disease in South-East Asia and the South-Western
studies have suggested a higher prevalence of kidney involvement
PLOS Neglected Tropical Diseases www.plosntds.org
January 2014 Volume 8 Issue 1 e2605
Scrub Typhus and Acute Kidney Injury
background, previous co-morbidities and treatment was taken
and complete physical examination was done in all patients to
A large number of patients present to Indian hospitals with
specifically look for presence of eschar, rash and lymphadenop-
acute febrile illness and multisystem involvement. Acute
athy. All routine hematological and biochemistry profiles were
kidney injury is an important component. Clinical mani-
noted at admission and follow up. Urine was tested using dipstick
festations do not allow distinction between infectious
for albumin and sugar, and microscopic examination of freshly
etiologies with overlapping presentations. Many of the
voided urine specimen was performed in all patients. Hourly urine
cases remain undiagnosed and therefore are not treated,
output and daily serum creatinine monitoring were done during
resulting in high mortality. Despite having all the elements
hospital stay. Complications were noted for all patients.
of endemicity, scrub tuphus, caused by the rickettsia andtransmitted to humans by the bites of trombiculid mite, is
not regognized in Indian hospitals due to non-availability
A confirmed case of scrub typhus was defined as the one with
of locally validated diagnostic tests. Previous reports have
positive nested PCR for O. tsutsugamushi with no other evidence of
been limited to serologyic testing, with high false positives
any other infection. As single point qualitative immunoglobulin
due to past exposure rather than acute infection.
M (IgM) enzyme linked immunosorbent assay (ELISA) has
Moreover, kidney involvement in this condition is not well
been extensively used to define cases of scrub typhus in published
known. We looked for scrub typhus DNA in 201 patientswith an acute febrile illness. About 25% tested positive;
literature especially from our region where the disease appears to
kidney involvement was seen in over 80%, and acute
be highly endemic, scrub typhus IgM antibody was also looked for
kidney injury in 53%. Acute kidney injury was a predictor of
in patients' sera by ELISA in all cases by commercially available
mortality. All these are new findings of public health
qualitative ELISA kit (InBios International, Inc., USA) according
importance and suggest the need to include testing for
to the manufacturer's instructions. The test was considered to
this condition in the diagnostic armanetarium and
be positive if the antibody was present at dilution of $1:100 as
development of local serological cutoffs.
defined by the manufacturer.
Shock was defined as systolic blood pressure ,90 mm Hg or
requirement of inotropes; acute respiratory distress syndrome
in this condition. These studies, however, have used either clinical
(ARDS) defined as PaO2/FiO2#300 mm Hg [17]; severe anemia
features alone or in combination with serology with single sample
as hemoglobin ,9 g/dL; leukocytosis as total leukocyte count .
arbitrary antibody titre cut offs [12] to make a diagnosis. Relia-
11000 cells/mL; leukopenia as total leukocyte count ,4000
bility on serology alone is problematic in endemic areas, and use of
cells/mL; thrombocytopenia as platelet count ,100000 cells/mL;
nucleic acid based testing (NAT) is recommended [13–15].
hypoalbuminemia as serum albumin ,3.5 g/dL; hyperbilirubin-
We prospectively studied the pattern of kidney involvement
emia as serum total bilirubin .1.2 mg/dL; elevated serum gluta-
and its impact on the outcome in scrub typhus patients who were
mate oxaloacetate aminotransferase (SGOT) as .40 U/L;
diagnosed by using a strict NAT based case definition.
elevated serum glutamate pyruvate aminotransferase (SGPT)as .40 U/L and elevated serum alkaline phosphatase (SAP) as
Materials and Methods
AKI was defined and staged according to Kidney Disease:
Improving Global Outcomes (KDIGO) definition [18].
The study was approved by the Institute Ethics Committee
of the Postgraduate Institute of Medical Education and Research.
Polymerase chain reaction for 56-kDa antigen of of
Written informed consent was obtained from all adult patients and
from the parents or legal guardians of minor subjects. The study
Genomic DNA was isolated from buffy coat of 5 ml blood
was conducted in accordance to the principles of the Declaration
collected in ethylenediaminetetraacetic acid (EDTA) vial using
of Helsinki.
QIA amp DNA mini kit according to manufacturer's instructions(Qiagen. Hilden, Germany). Nucleotide specific sequence ampli-
Study setting and subjects
fication was done for the presence of 56-kDa antigen of of
This study was done at the Nehru Hospital of Postgraduate
O. tsutsugamushi. A set of nested PCR primers were used for two
Institute of Medical Education and Research, the largest tertiary
rounds of amplification (outer primers, forward: TCAAGCT-
care referral hospital in North India located near the foothills of
TATTGCTAGTGCAATGTCTGC, reverse: AGGGATCCCT-
The Great Himalayas. From September 2011 to November 2012,
GCTGCTGTGCTTGCTGCG; inner primers, forward: GAT-
all patients referred to our hospital with unexplained fever and/or
CAAGCTTCCTCAGCCTACTATAATGCC, reverse: CTAG-
varying degrees of multisystem involvement were tested for O.
GGATCCCGACAGATGCACTATTAGGC) using conditions
tsutsugamushi deoxyribonucleic acid (DNA) in blood by nested
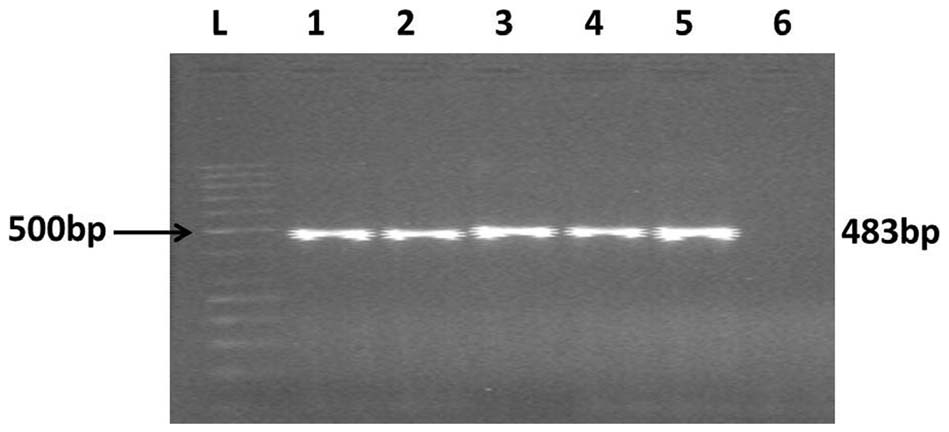
described earlier [16,19]. Visualization of specific 483 bp ampli-
polymerase chain reaction (PCR) targeting gene encoding for the
fication product was considered to be diagnostic (Figure 1).
56-kDa antigen of Gilliam strain of O. tsutsugamushi [16].
A previously confirmed scrub typhus patient sample (fever with
All patients also underwent at least three blood cultures for
eschar, $4 fold rise in IgM antibody titres by enzyme linked
bacterial growth, three peripheral blood film examinations for
immunosorbent assay and positive nested PCR for gene encoding
malarial parasite and malarial antigen detection in blood by
56-kDa antigen of O. tsutsugamushi confirmed by sequencing)
immunochromatographic rapid card test (QDx Malaria PAN/Pf
was taken as positive control. For each run, one positive human
and Pv/Pf, Piramal Healthcare, India). In addition, dengue virus
control, one healthy negative human control and one negative
NS1 antigen, dengue virus IgM antibody and leptospiral IgM
control (without any DNA) were run simultaneously to confirm the
antibody were tested in blood samples of all patients.
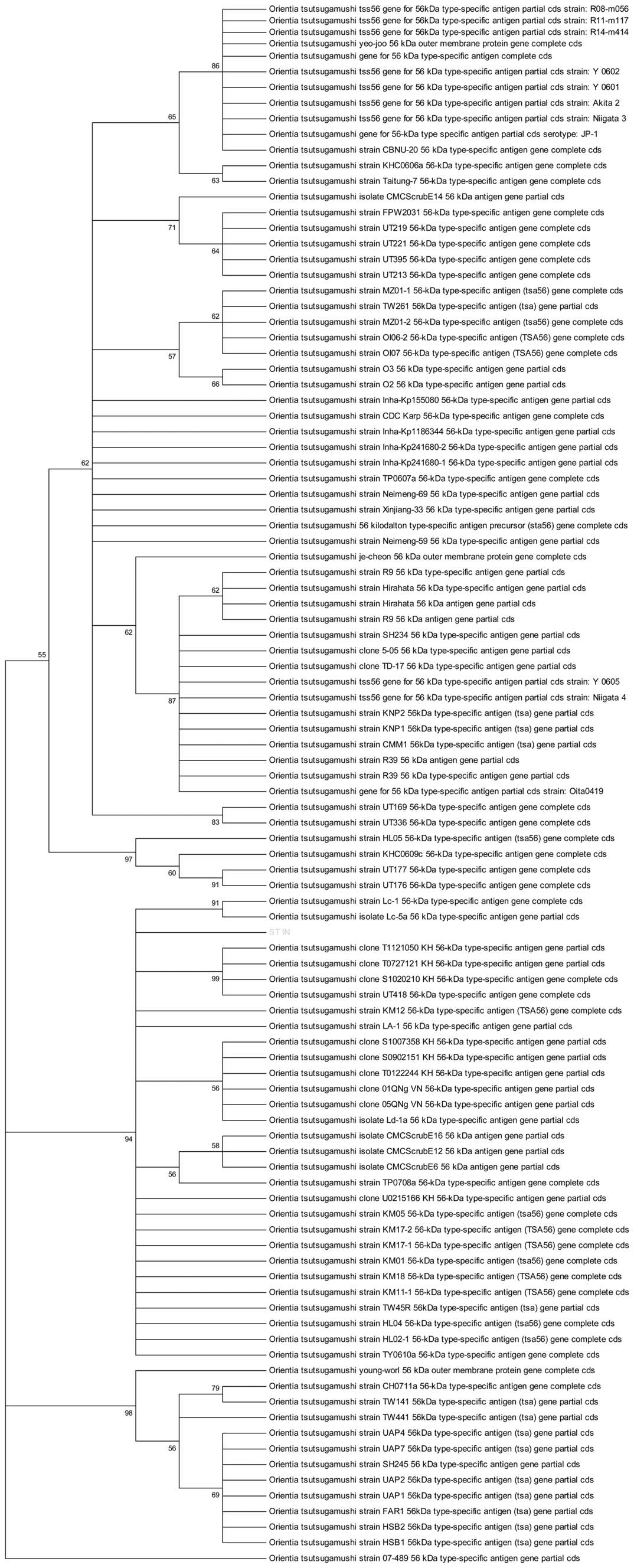
accuracy. Sequencing of PCR product was done in 3 randomly
Demographic details and clinical course were recorded for
selected patients. Sequence alignment was done with nucleotide
all patients. A detailed history which included recording of signs
blast on pubmed and analyzed using Molecular Evolutionary
and symptoms, occupational details, geographic and social
Genetics Analysis (MEGA) software for phylogenetic tree analysis.
PLOS Neglected Tropical Diseases www.plosntds.org
January 2014 Volume 8 Issue 1 e2605
Scrub Typhus and Acute Kidney Injury
diagnosed during summer months from March to June. Majorityof the cases occurred after rainy season in July–August andcontinued through winter.
Table 3 lists the clinical manifestations recorded in this
study population. In addition to fever, the main symptoms wereshortness of breath, jaundice, pain abdomen, vomiting, decreasedurine output, headache and altered mentation. Tachycardia,hepatomegaly, tachypnea and splenomegaly were noted in 73%,69%, 67% and 41% of the patients, respectively. Eschar was notedin 9 cases; the location being chest (3) and nape of neck, arm,index finger of hand, hypogastric region, gluteal region and
Figure 1. The ethidium bromide-stained agarose gel shows
popliteal fossa. Amongst these confirmed cases, IgM ELISA for
the 483 bp polymerase chain reaction products. L: 500 bp
scrub typhus was positive in 80%.
ladder, 1–4: patients' samples; 5: positive control; 6: negative control.
Renal abnormalities were noted in 82% of the scrub typhus
patients (Table 4). Abnormal urinalysis was present in 61%, themajor abnormalities being dipstick positive albuminuria (55%)
The results showed .98% homology with O. tsutsugamushi family
and microscopic hematuria (16%). AKI, as defined according to
strains (Figure 2, test sequence highlighted). This nested PCR was
KDIGO definition, was seen in 53% of patients. A total of 5 (10%)
also performed on eschar tissue scraped from 2 patients who had
patients were in stage 1, 4 (8%) in stage 2 and 17 (35%) in stage 3.
positive blood samples.
Jaundice, oliguria and mortality were significantly more in patientswith AKI (Table 3). About half of all patients with AKI were
oliguric. There were no significant differences between the oliguric
The patients were treated with either doxycycline (100 mg twice
and non-oliguric scrub typhus patients with AKI except for mor-
daily for 7 days) or azithromycin (500 mg daily for 3 days). Fluid
tality which was significantly higher in oliguric patients (p = 0.011).
overload, hyperkalemia or metabolic acidosis refractory to medical
Gross, painless hematuria was seen in two patients, and one had
measures, or persistent oliguria were indications for starting
intravascular hemolysis. A 14-year-old male who presented with
fever and gross hematuria underwent a kidney biopsy that showedmesangial hypercellularity with 2+ mesangial deposition of
immunoglobulin A (IgA). He continued to have microscopic
Urinalysis abnormalities and AKI were the outcomes of interest.
hematuria after 6 months. One patient had nephrotic range pro-
The study population was divided into two groups based on
teinuria at presentation that rapidly improved over 2 weeks and
presence or absence of AKI.
hence, biopsy was not done. Three patients required dialysis.
Prominent hematological abnormalities included thrombocy-
Statistical analysis
topenia, leucocytosis and severe anemia (Table 3). Hyperbi-
Data was analysed using Statistical Package for the Social
lirubinemia, transaminitis, and hypoalbuminemia were also seen
Sciences (SPSS) software for Windows, version 20.0 (IBM Corp.,
in majority of patients. Over 50% patients developed ARDS.
Armonk NY). Univariate analysis was done to assess association
Secondary hemophagocytosis and septic arthritis were seen in
of various parameters with presence of AKI and final outcome.
one patient each. Interestingly, two of the patients were kidney
Binary logistic regression analysis (forward conditional) was used to
look for independent association of clinical and laboratory factors
Patients with characteristic eschar were immediately started on
with the outcome. All p values were two-tailed, and considered to
treatment once blood samples were collected for testing. Other-
be significant at ,0.05.
wise, specific treatment for scrub typhus was started only afterdiagnosis was confirmed. The disease was fatal in 8 patients, all of
whom had ARDS and AKI. All three patients who requireddialysis expired. On univariate analysis, jaundice, oliguria,
Out of 201 patients with fever and multisystem involvement
elevated bilirubin, elevated SGOT, elevated SGPT, ARDS and
seen during this period, 49 tested positive for O. tsutsugamushi DNA.
AKI were significantly associated with mortality (p of 0.045,
None of these had any alternative diagnosis (Table 1). Amongst
0.0001, 0.005, 0.022, 0.039, 0.007 and 0.004, respectively). There
152 patients who were negative for scrub typhus by aforemen-
was no significant association of stage of AKI with mortality
tioned PCR, 20% patients had an alternative diagnosis (Table 2).
(p = 0.214). On multivariate analysis, only oliguric AKI showed an
Importantly, a total of 105 patients were recorded as positive for
independent association with mortality (p = 0.002, Cox & Snell R
scrub typhus IgM ELISA. These included 43% of scrub typhus
Square 0.309).
PCR negative patients. A total of 23% of patients within this
Except the person with persistent hematuria, all surviving
subset (scrub typhus PCR negative but IgM ELISA positive) were
patients had normal renal function and normal urinalysis at 3
assigned an alternative diagnosis. A comparison of the clinical
months after recovery.
features and laboratory abnormalities in scrub typhus positive andnegative patients is given in Table 1. Vomiting, altered sensorium,
bodyaches, tachycardia, hepatomegaly, lymphadenopathy, AKIand thrombocytopenia were significantly more common in
This is the first report to comprehensively document the clinical
patients with scrub typhus (Table 1).
picture, investigative profile, pattern of renal involvement and
Males constituted 59% of the scrub typhus PCR positive cases.
outcome in a cohort of patients of scrub typhus using a strict case
The mean age was 34.1614.4 (range 11–65) years and the
definition. We show that scrub typhus is responsible for about 24%
duration of symptoms at presentation was 10.864.9 (range 3–30)
of all patients presenting with unexplained febrile illness and/
days. About 84% patients were from rural areas. No cases were
or multi-system involvement. We also show that the renal
PLOS Neglected Tropical Diseases www.plosntds.org
January 2014 Volume 8 Issue 1 e2605
Scrub Typhus and Acute Kidney Injury
Figure 2. Phylogenetic tree analysis, highlighted test sample shows .98% homology to O. tsutsugamushi.
doi:10.1371/journal.pntd.0002605.g002
PLOS Neglected Tropical Diseases www.plosntds.org
January 2014 Volume 8 Issue 1 e2605
Scrub Typhus and Acute Kidney Injury
Table 1. Clinical and laboratory manifestations in patients (total no. of patients: 201).
Scrub typhus (n = 49)
Shortness of breath
Decreased urine output
Altered sensorium
Bleeding manifestations
Hemoglobin (g/dL)
Platelet count (per mL)
Serum total bilirubin (mg/dL)
Total protein (g/dL)
Serum albumin (g/dL)
Serum creatinine (mg/dL)
Scrub typhus IgM ELISA positivity
AKI: acute kidney injury, ARDS: acute respiratory distress syndrome, ELISA: enzyme linked immunosorbent assay, IgM: immunoglobulin M, PCR: polymerase chainreaction, SAP: serum alkaline phosphatase SGOT: serum glutamate oxaloacetate aminotransferase, SGPT: serum glutamate pyruvate aminotransferase, TLC: totalleukocyte count.
doi:10.1371/journal.pntd.0002605.t001
involvement is fairly common in scrub typhus. AKI is seen in over
Scrub typhus does not find a mention in most descriptions of
50% cases, and is an important predictor of mortality.
tropical community acquired AKI. In part, the reason has been
Scrub typhus is caused by obligate, intracellular bacterium
inability to make an accurate diagnosis. The clinical description
O. tsutsugamushi which is maintained in nature by trans-ovarian
lays emphasis on the presence of an eschar, which is often difficult
transmission in trombiculid mites. Human involvement occurs
to see in dark-skinned persons. Supporting tests include either
accidentally when they get bitten by infected trombiculid mite
demonstration of rising antibody titre or rickettsial DNA [15].
larvae (chiggers) leading to inoculation of organisms into skin.
Serologic tests are plagued by under-reporting of methodology and
Vascular endothelial cell injury leading to vasculitis is the pre-
variable seropositivity criteria. [15,20]. Most Indian reports have
dominant mechanism of cellular injury in this disease.
relied on a single point commercially available IgM ELISA using
PLOS Neglected Tropical Diseases www.plosntds.org
January 2014 Volume 8 Issue 1 e2605
Scrub Typhus and Acute Kidney Injury
and murine typhus patients. Also, the investigators showed that
Table 2. Diagnoses in scrub typhus PCR negative population.
this PCR amplified DNA of 9 other strains of O. tsutsugamushiprevalent in South-East Asia and suggested that it could be used todetect diverse antigenic types of O. tsutsugamushi. In a study from
Scrub typhus IgM ELISA
Korea, nested PCR for gene encoding the 56 kDa antigen of
O. tsutsugamushi was shown to have a sensitivity of 82.2% and a
specificity of 100% when compared with IFA (diagnosis made byeither single point titres cut off or four fold rise in titres in
convalescent sera) [26]. In another recent study from the same
centre where the investigators compared various types of PCR
(47 kDa gene, 56 kDa gene) for scrub typhus diagnosis (confirmed
Pyogenic meningitis
only by four fold rise in convalescent sera titres by IFA), 56 kDa
nested PCR was found to have the highest sensitivity (87.8%)
and 100% specificity [14]. IFA which is considered current goldstandard reference diagnostic method is imperfect, gives retro-
Japanese encephalitis
spective diagnosis and plagued by variability in methodology and
arbitrarily defined cut off titres without supporting epidemiological
data [23]. Theoretically, PCR based assays would offer diagnosis
till bacteremia persists, before antibody response occurs in earlyphase of disease and overcome the problem of high background
*Drug Reaction with Eosinophila and Systemic Symptoms (DRESS);#
titres in endemic areas before antibody response starts appearing.
Still's disease, erythema nodosum, polymyositis, dapsone syndrome,
However, once bacteremia has cleared with or without treatment,
ELISA: enzyme linked immunosorbent assay, IgM: immunoglobulin M, PCR:
PCR based assays would be negative. Therefore, it has been
polymerase chain reaction.
suggested that future diagnostic development should preferably
focus on both pathogen and antibody based tests [23]. Recently, aset of robust set of reference criteria comprising culture, serological
cutoffs that have been derived from low endemicity areas. A major
cut offs backed by local epidemiological data and combination of
limiting factor is lack of availability of local seroprevalence dats.
various available PCRs has been proposed for validation of new
Single time point estimations should be used only when robust
diagnostic techniques for scrub typhus [21].
local seroprevalence data is available [14,20]. Variable single point
Therefore, our study appropriately highlights the current limi-
titres in India ($1:100, $16 units) and Thailand ($1:400) have
tations of using such serologic tests for diagnosis of scrub typhus
been reported as positive [6,8,13]. However, using serology alone,
and suggests the need to obtain robust population data to deter-
Paris et al used an admission IgM titer of $1:12,800 (based on
mine appropriate cutoffs for diagnosis. Antibody titre estimation in
local seroprevalence data and highest titres seen during acute
paired serum samples may overcome these limitations, but the
infections) or a four-fold rise in IgM antibody by immunofluores-
diagnosis would be retrospective in such a situation and may not
cence antibody assay (IFA) to define a case of scrub typhus in
help in immediately guiding treatment.
Thailand [21]. Therefore, use of single sample titres for making a
Using this nested PCR as confirmatory diagnostic criterion,
positive diagnosis using arbitrary cutoff without local validation is
24% of patients with unexplained febrile illness seen at our centre
strongly discouraged [15,22,23]. Unfortunately, seroprevalence
had scrub typhus. In a study from South India [27], about 51% of
data in Indian population is not available. Our study shows
all patients with febrile illness were diagnosed as scrub typhus on
that diagnosis of scrub typhus using single time qualitative IgM
the basis of ELISA. It is important to note that there is no data
antibody estimation by the commercially available IgM ELISA kit
from Indian population which validates antibody titre cutoffs
would have failed to diagnose scrub typhus in 20% of PCR
put forward by manufacturer's in Western countries. Had we also
positive confirmed cases.
based the diagnosis on serology, the prevalence would have been
Nested PCR targeting gene encoding for the 56-kDa antigen of
57%. We did not note any geographic clustering. The condition
Gilliam strain of O. tsutsugamushi has been shown to have high
was also seen in urban residents,who are traditionally considered
sensitivity and specificity. This primer set has been shown to
to be at low risk [28,29]. Whether this is related to environment,
amplify DNA sequences from other strains of O. tsutsugamushi
host, pathogen or vector related factors needs further studies.
[13,16,24,25], and has been suggested as a group specific test for
Epidemiological investigation of a recent outbreak of scrub typhus
O. tsutsugamushi [13]. Importantly, this PCR has been shown to be
in North-East India suggested emergence of a new species of
negative in normal humans and other infections. It is important to
vector trombiculid mite, Schoengastiella ligula [30]. The increased
note that the serotype specific primers are different from this
incidence after rainy season is expected as increased vegetation
set and have been described in literature [16]. In a study of 36
after rains support growth of larvae of trombiculid mite, reflecting
patients who presented with fever at a large provincial hospital in
tropical disease epidemiology. There is a trend towards more use
Southern Thailand, nested PCR for gene encoding the 56 kDa
of fluoroquinolone, cephalosporins, extended spectrum penicillins
antigen of Gilliam strain of O. tsutsugamushi was compared with IFA
and newer antibiotics in the community [31,32]. We believe that
(both acute and convalescent sera in only 17 patients) [13]. This
increasing use of these antibiotics for treatment of febrile illnesses
PCR detected all 9 patients who were diagnosed by serology
in the community during recent times may be contributing to
(positive if single point titre of .1:400 or a four-fold rise in titre to
unmasking of this disease as the causative organism is inherently
at least 1:200), and in addition was positive in 3 more patients who
resistant to them.
were negative by serology. The reported range for days after onset
Till recently, renal involvement due to scrub typhus had not
of disease and specific drug treatment when samples were taken
received much attention. A recent systematic review could only
for testing ranged from 5–33 days and 1–27 days, respectively.
find a few case reports specifically describing acute renal failure
Importantly, this PCR was negative in healthy human controls
due to scrub typhus [33]. Overall, renal involvement is considered
PLOS Neglected Tropical Diseases www.plosntds.org
January 2014 Volume 8 Issue 1 e2605
Scrub Typhus and Acute Kidney Injury
Table 3. Comparison of clinical, laboratory manifestations and complications in the AKI and non-AKI groups in the confirmedscrub typhus study population (scrub typhus PCR positive, no. of patients: 49).
P value (two tailed)
Shortness of breath
Altered sensorium
Bleeding manifestations
Hemoglobin (g/dL)
Platelet count (per mL)
Serum total bilirubin (mg/dL)
Total protein (g/dL)
Serum albumin (g/dL)
Blood urea (mg/dL)
Serum creatinine (mg/dL)
Scrub typhus IgM ELISA positivity
PLOS Neglected Tropical Diseases www.plosntds.org
January 2014 Volume 8 Issue 1 e2605
Scrub Typhus and Acute Kidney Injury
Table 3. Cont.
P value (two tailed)
AKI: acute kidney injury, ARDS: acute respiratory distress syndrome, ELISA: enzyme linked immunosorbent assay, IgM: immunoglobulin M, PCR: polymerase chainreaction, SAP: serum alkaline phosphatase SGOT: serum glutamate oxaloacetate aminotransferase, SGPT: serum glutamate pyruvate aminotransferase, TLC: totalleukocyte count.
doi:10.1371/journal.pntd.0002605.t003
to be a part of multi-organ dysfunction syndrome in patients with
expired. This may be a reflection of underlying severity of disease.
severe disease [10,11]. In Taiwan, incidence of AKI in scrub
The significant association of hyperbilirubinemia with AKI and
typhus was reported to be 8.3% and 6.6% in two series [34,35].
association of increased mortality with oliguric form of AKI
Importantly, clinical course in 8 out of 9 patients who developed
may also be a reflection of the same. Basu et al [27] also showed
acute renal failure in one of these series was complicated by septic
increasing mortality risk with increasing severity of AKI.
shock which might have precipitated AKI [34]. In India, two series
There are some limitations to this study. Our study population
from South India have shown the incidence of AKI to be 19% and
is unlikely to represent the true burden of this disease as only those
42% (Table 5) [6,27,36,37]. A recent series from North India
patients who had severe disease or were unresponsive to treatment
reported AKI in 34% patients [8]. It is important to note that that
in community health facilities would have been referred to our
the basis of diagnosis has been a single point measurement of
tertiary care centre. Secondly, the diagnosis was based on a single
antibody using an arbitrary cutoff, and therefore subject to the
nucleic acid test. Other nucleic acid-based tests such as 47-
above mentioned limitations. Our study is the first to use a robust
kDa-based and GroEL-based real-time PCR and loop-mediated
diagnostic parameter to identify definitive cases and evaluate renal
isothermal PCR [20] have also been used. It is possible that a
combination of these along with culture and properly validated
Renal abnormalities were present in 82% cases, and .50%
local serological criteria would allow identification of more cases.
patients had AKI. Abnormal urinalysis was seen in 61% of
Despite these limitation, our current observations are significant
patients. In a study from Vietnam, abnormal urinalysis, almost
as they identify scrub typhus as an important cause of unexplained
exclusively proteinuria, was reported in 20% of patients with scrub
acute febrile illness in this region and contradict the current notion
typhus diagnosed by IFA or mouse inoculation methods [38].
that AKI is uncommon complication in this disease. Whether the
Mild proteinuria or microscopic hematuria have been reported in
higher incidence of AKI in hospitalized patients with scrub typhus
scrub typhus patients with acute renal failure [39]. A recent study
in our region compared to that reported from other centres is
from India reported abnormal urinalysis in 57% patients [36].
actually related to some host factor, differences in microbial
Low-grade albuminuria, along with microscopic hematuria, pyuriaand glucosuria suggest predominant tubulo-interstitial involve-ment. Clinical evidence of glomerular involvement was seen in 2
Table 4. Renal abnormalities in the confirmed scrub typhus
cases, one as nephrotic range proteinuria that improved sponta-
study population (no. of patients: 49).
neously, and the other with glomerular hematuria who was shownto have IgA nephropathy on biopsy. It is likely that concurrentfebrile illness due to scrub typhus precipitated episode of gross
No. of patients (%)
hematuria in the second patient.
Oliguria (,400 ml/d)
Other descriptions of acute renal failure in scrub typhus are
in the form of case reports [39–43] and one autopsy study [44].
The mechanism of AKI in scrub typhus is mainly believed to
be impaired renal perfusion due to volume depletion or increased
vascular permeability [42]. Other potential mechanisms include
Abnormal urinalysis
direct tubular toxicity leading to acute tubular necrosis, interstitial
Dipstick positive albuminuria
nephritis, pigment nephropathy due to rhabdomyolysis andthrombotic microangiopathy secondary to disseminated intravas-
cular coagulation. Renal biopsies have shown mild mesangial
hyperplasia, acute tubular necrosis or tubulointerstitial nephritis
[40,42,45]. The autopsy series published 67 years back described
Dipstick positive glucosuria
renal histopathologic changes in 69 patients with scrub typhus
Significant pyuria (.9 pus cells/hpf)
[44]. Proximal tubular epithelial swelling and interstitial nephritis
Microscopic hematuria (.2 RBC/hpf)#
were universal. Focal or diffuse glomerulonephritis was seen in
30% of kidney specimens. Fibrin filled capillaries or swollenendothelial cells leading to glomerular ischemia was another
prominent observation. Kidneys were the second most common
site of vascular changes after testes. Evidently, these findings
represented involvement in severest form which led to death of
excludes two patients with gross hematuria;
$defined according to KDIGO guidelines for AKI.
In our study, the outcome of AKI was largely favourable as all
AKI: acute kidney injury, KDIGO: Kidney Disease: Improving Global Outcomes,
the surviving patients with AKI had completely recovered their
RBC: red blood cell.
renal function. All 3 patients who had dialysis dependent AKI
PLOS Neglected Tropical Diseases www.plosntds.org
January 2014 Volume 8 Issue 1 e2605
Scrub Typhus and Acute Kidney Injury
Table 5. Renal involvement in scrub typhus.
35, age #12 years
20% of all patients (stages
1, 2 and 3 reported as 29%,
42% and 29% of all patientswith AKI, respectively)
188, age $18 years
42.6% of all patients (risk,
injury and failure in 48%,26% and 26% of all patientswith AKI, respectively)
189, age $16 years
19.6% of all patients
259, median age 39
23.2% of all patients (risk,
injury and failure in 38%,22% and 40% of all patientswith AKI, respectively)
515, only data about
35% of all patients (risk,
patients with AKI
injury and failure in 45%,
presented (mean age
34% and 21% of all patients
with AKI, respectively)
136, age $2 years
$0.5 mg/dL increase
6.6% of all patients
in serum creatinineover baseline orlowest value OR24 hour urinevolume ,400 ml
*Used $4 fold rise in antibody titre in paired serum samples if diagnosed by IFA.
AKIN: Acute Kidney Injury Network, ELISA: Enzyme Linked Immunosorbent Assay, IgM: Immunoglobulin M.
doi:10.1371/journal.pntd.0002605.t005
virulence or is an actual unmasking of a previously unrecognized
Supporting Information
complication is difficult to infer due to variability and paucityof existing literature. Standardization of diagnostic criteria and
STROBE checklist.
uniform definitions of various manifestations when applied across
various centres may help in this regard.
In conclusion, scrub typhus is an important cause of febrile
Author Contributions
illness with multisystem involvement in tropical regions. Renal
Conceived and designed the experiments: VivK VJ. Performed the
involvement is common and AKI is an independent predictor of
experiments: VinK AKY SI. Analyzed the data: VivK VinK AKY SI RA.
mortality. We suggest that the panel of investigation in all these
Contributed reagents/materials/analysis tools: AB NS SJ. Wrote the
cases should include PCR for O tsutsugamushi. The discrepancy
paper: VivK AKY VJ.
between NAT positivity and IgM ELISA positivity as definedby arbitrary cutoffs suggests the need to develop robust localseroprevalence data.
1. WHO Recommended Surveillance Standards WHO/CDS/CSR/ISR/99.2.
8. Vikrant S, Dheer SK, Parashar A, Gupta D, Thakur S, et al. (2013) Scrub
Second ed: World Health Organization. Available from: http://www.who.int/
typhus associated acute kidney injury—a study from a tertiary care hospital from
western Himalayan state of India. Renal Failure: 1–6.
2. Watt G, Parola P (2003) Scrub typhus and tropical rickettsioses. Curr Opin
9. John TJ, Dandona L, Sharma VP, Kakkar M (2011) Continuing challenge of
Infect Dis 16: 429–436.
infectious diseases in India. Lancet 377: 252–269.
3. Sharma A, Mahajan S, Gupta ML, Kanga A, Sharma V (2005) Investigation of
10. Raoult D (2009) Orientia tsutsugamushi (Scrub Typhus). In: Mandell GL, Bennett
an outbreak of scrub typhus in the himalayan region of India. Jpn J Infect Dis
JE, Dolin R, editors. Mandell: Mandell, Douglas, and Bennett's Principles and
58: 208–210.
Practice of Infectious Diseases. Seventh ed: Churchill Livingstone, An Imprint of
4. Vivekanandan M, Mani A, Priya YS, Singh AP, Jayakumar S, et al. (2010)
Elsevier. pp. 2529–2530.
Outbreak of scrub typhus in Pondicherry. J Assoc Physicians India 58: 24–28.
11. Reller ME, Dumler JS (2011) Scrub Typhus (Orientia tsutsugamushi). In: Kliegman
5. Khan SA, Dutta P, Khan AM, Topno R, Borah J, et al. (2012) Re-emergence of
RM, Stanton BF, GemeIII JWS, Schor NF, Behrman RE, editors. Kliegman:
scrub typhus in northeast India. Int J Infect Dis 16: e889–890.
Nelson Textbook of Pediatrics. Nineteenth ed: Saunders, An Imprint of Elsevier.
6. Chrispal A, Boorugu H, Gopinath KG, Prakash JA, Chandy S, et al. (2010)
pp. 1045–1046.
Scrub typhus: an unrecognized threat in South India - clinical profile and
12. Chogle AR (2010) Diagnosis and treatment of scrub typhus–the Indian scenario.
predictors of mortality. Trop Doct 40: 129–133.
J Assoc Physicians India 58: 11–12.
7. Varghese GM, Abraham OC, Mathai D, Thomas K, Aaron R, et al. (2006)
13. Saisongkorh W, Chenchittikul M, Silpapojakul K (2004) Evaluation of nested
Scrub typhus among hospitalised patients with febrile illness in South India:
PCR for the diagnosis of scrub typhus among patients with acute pyrexia of
magnitude and clinical predictors. J Infect 52: 56–60.
unknown origin. Trans R Soc Trop Med Hyg 98: 360–366.
PLOS Neglected Tropical Diseases www.plosntds.org
January 2014 Volume 8 Issue 1 e2605
Scrub Typhus and Acute Kidney Injury
14. Kim DM, Park G, Kim HS, Lee JY, Neupane GP, et al. (2011) Comparison of
29. Wang YC, Chen PC, Lee KF, Wu YC, Chiu CH (2013) Scrub typhus cases in a
conventional, nested, and real-time quantitative PCR for diagnosis of scrub
teaching hospital in Penghu, Taiwan, 2006–2010. Vector Borne Zoonotic Dis
typhus. Journal of clinical microbiology 49: 607–612.
13: 154–159.
15. Richards AL (2012) Worldwide detection and identification of new and
30. Tilak R, Kunwar R, Wankhade UB, Tilak VW (2011) Emergence of
old rickettsiae and rickettsial diseases. FEMS Immunol Med Microbiol 64:
Schoengastiella ligula as the vector of scrub typhus outbreak in Darjeeling:
has Leptotrombidium deliense been replaced? Indian J Public Health 55: 92–99.
16. Furuya Y, Yoshida Y, Katayama T, Yamamoto S, Kawamura A, Jr. (1993)
31. Chandy SJ, Thomas K, Mathai E, Antonisamy B, Holloway KA, et al. (2013)
Serotype-specific amplification of Rickettsia tsutsugamushi DNA by nested
Patterns of antibiotic use in the community and challenges of antibiotic
polymerase chain reaction. Journal of clinical microbiology 31: 1637–1640.
surveillance in a lower-middle-income country setting: a repeated cross-sectional
17. Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al.
study in Vellore, South India. J Antimicrob Chemother 68: 229–236.
(2012) Acute respiratory distress syndrome: the Berlin Definition. JAMA 307:
32. Kotwani A, Holloway K (2011) Trends in antibiotic use among outpatients in
New Delhi, India. BMC Infect Dis 11: 99.
18. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury
33. Rajapakse S, Rodrigo C, Fernando D (2012) Scrub typhus: pathophysiology,
Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury.
clinical manifestations and prognosis. Asian Pac J Trop Med 5: 261–264.
Kidney inter., Suppl. 2012; 2: 1–138
34. Wu K-M, Wu Z-W, Peng G-Q, Wu JL, Lee S-Y (2009) Radiologic Pulmonary
19. Kwok S, Higuchi R (1989) Avoiding false positives with PCR. Nature 339:
Findings, Clinical Manifestations and Serious Complications in Scrub Typhus:
Experiences From A Teaching Hospital in Eastern Taiwan. InternationalJournal of Gerontology 3: 223–232.
20. Blacksell SD, Bryant NJ, Paris DH, Doust JA, Sakoda Y, et al. (2007) Scrub
35. Tsay RW, Chang FY (1998) Serious complications in scrub typhus. J Microbiol
typhus serologic testing with the indirect immunofluorescence method as a
Immunol Infect 31: 240–244.
diagnostic gold standard: a lack of consensus leads to a lot of confusion. Clin
36. Attur RP, Kuppasamy S, Bairy M, Nagaraju SP, Pammidi NR, et al. (2013)
Infect Dis 44: 391–401.
Acute kidney injury in scrub typhus. Clin Exp Nephrol 17 : 725–729.
21. Paris DH, Blacksell SD, Nawtaisong P, Jenjaroen K, Teeraratkul A, et al. (2011)
37. Kumar M, Krishnamurthy S, Delhikumar CG, Narayanan P, Biswal N, et al.
Diagnostic accuracy of a loop-mediated isothermal PCR assay for detection of
(2012) Scrub typhus in children at a tertiary hospital in southern India: clinical
Orientia tsutsugamushi during acute Scrub Typhus infection. PLoS Neglected
profile and complications. J Infect Public Health 5: 82–88.
Tropical Diseases 5: e1307.
38. Berman SJ, Kundin WD (1973) Scrub typhus in South Vietnam. A study of 87
22. Koh GC, Maude RJ, Paris DH, Newton PN, Blacksell SD (2010) Diagnosis of
cases. Ann Intern Med 79: 26–30.
scrub typhus. The American journal of tropical medicine and hygiene 82:
39. Yen TH, Chang CT, Lin JL, Jiang JR, Lee KF (2003) Scrub typhus: a frequently
overlooked cause of acute renal failure. Ren Fail 25: 397–410.
23. Paris DH, Shelite TR, Day NP, Walker DH (2013) Unresolved problems related
40. Hsu GJ, Young T, Peng MY, Chang FY, Chou MY, et al. (1993) Acute renal
to scrub typhus: a seriously neglected life-threatening disease. The American
failure associated with scrub typhus: report of a case. J Formos Med Assoc 92:
journal of tropical medicine and hygiene 89: 301–307.
24. Furuya Y, Yoshida Y, Katayama T, Kawamori F, Yamamoto S, et al. (1991)
41. Lee S, Kang KP, Kim W, Kang SK, Lee HB, et al. (2003) A case of acute renal
Specific amplification of Rickettsia tsutsugamushi DNA from clinical specimens by
failure, rhabdomyolysis and disseminated intravascular coagulation associated
polymerase chain reaction. Journal of clinical microbiology 29: 2628–2630.
with scrub typhus. Clin Nephrol 60: 59–61.
25. Ohashi N, Nashimoto H, Ikeda H, Tamura A (1990) Cloning and sequencing of
42. Kim DM, Kang DW, Kim JO, Chung JH, Kim HL, et al. (2008) Acute
the gene (tsg56) encoding a type-specific antigen from Rickettsia tsutsugamushi.
renal failure due to acute tubular necrosis caused by direct invasion of Orientia
Gene 91: 119–122.
tsutsugamushi. Journal of clinical microbiology 46: 1548–1550.
26. Kim DM, Yun NR, Yang TY, Lee JH, Yang JT, et al. (2006) Usefulness of
43. Young PC, Hae CC, Lee KH, Hoon CJ (2003) Tsutsugamushi infection-
nested PCR for the diagnosis of scrub typhus in clinical practice: A prospective
associated acute rhabdomyolysis and acute renal failure. Korean J Intern Med
study. The American journal of tropical medicine and hygiene 75: 542–545.
18: 248–250.
27. Basu G, Chrispal A, Boorugu H, Gopinath KG, Chandy S, et al. (2011) Acute
44. Allen AC, Spitz S (1945) A Comparative Study of the Pathology of Scrub
kidney injury in tropical acute febrile illness in a tertiary care centre–RIFLE
Typhus (Tsutsugamushi Disease) and Other Rickettsial Diseases. Am J Pathol
criteria validation. Nephrol Dial Transplant 26: 524–531.
21: 603–681.
28. Li PK-T, Burdmann EA, Mehta RL (2013) Acute kidney injury: Acute kidney
45. Chi WC, Huang JJ, Sung JM, Lan RR, Ko WC, et al. (1997) Scrub typhus
injury[mdash]global health alert. Nat Rev Nephrol [epub ahead of print].
associated with multiorgan failure: a case report. Scand J Infect Dis 29: 634–635.
PLOS Neglected Tropical Diseases www.plosntds.org
January 2014 Volume 8 Issue 1 e2605
Source: http://www.georgeinstitute.org.in/sites/default/files/scrub-typhus-plos-paper.pdf
Diagnosis and Management of Hypothermia in Neurosurgical Patients By Avery Jackson, MD Dear Colleagues: I came across an article that I wanted to share with you that was put together by Powers and Friedman out of Duke University Department of Neurosurgery regarding hyponatremia. It is in Contemporary Neurosurgery. I found it to be extremely helpful in the management of hyponatremia. Hyponatremia is a common complication of subarachnoid hemorrhage, brain tumors and cerebral infections. Hormonal factor such as Natriuretic Peptides and Antidiuretic Hormone play important roles in hyponatremia and neurosurgical patients. It is important to differentiate between cerebral salt-wasting (CSW) and syndrome of inappropriate secretion of antidiuretic hormone (SIADH).
The water-en e ergy-em Tamara Jackson IAL Travel Fellowship 2009 CONTENTS Acknowledgements . 3 Background to study topic . 4 The Australian situation . 7 Irrigation industry . 10 Observations . 11 Agricultural energy consumption . 11 State of technology & importance of energy issues . 14 Irrigation industry . 16


