
Cialis ist bekannt für seine lange Wirkdauer von bis zu 36 Stunden. Dadurch unterscheidet es sich deutlich von Viagra. Viele Schweizer vergleichen daher Preise und schauen nach Angeboten unter dem Begriff cialis generika schweiz, da Generika erschwinglicher sind.
Theheal.ca
Osteoporos Int (2014) 25:205–210DOI 10.1007/s00198-013-2453-z
Comparison of hip fracture and osteoporosis medicationprescription rates across Canadian provinces
R. G. Crilly & M. Kloseck & B. Chesworth & S. Mequanint &E. Sadowski & J. Gilliland
Received: 2 April 2013 / Accepted: 14 June 2013 / Published online: 2 August 2013
# International Osteoporosis Foundation and National Osteoporosis Foundation 2013
monthly, and yearly, medication prescriptions were converted
Summary The study explores osteoporosis medication pre-
to "units" of prescribing, so that a once a year infusion repre-
scribing across Canadian provinces and any impact on hip
sented 365 units, a monthly prescription 30 units, and so forth.
fracture rates. Despite a marked variation in the prescribing
Results There is a fourfold difference in prescribing across
of such medication, there is no effect on the hip fracture rate
provinces but no corresponding variation in hip fracture rate.
in either gender or any age group, suggesting either poor
No significant correlation exists between prescribing load and
targeting or lack of efficacy.
hip fracture rate. This was true for all age groups, both genders,
Introduction Hip fractures are the most disabling and costly
and for both intertrochanteric and subcapital hip fracture.
of osteoporotic fractures, and a reduction in the risk of hip
Conclusions We find no association between osteoporosis
fracture is an expectation of osteoporosis medications. In this
medication prescribing and hip fracture rate. Possible expla-
study, we have compared the use of osteoporosis medication
nations include insufficient numbers of at-risk patients on
across Canadian provinces with the rate of hip fractures in
treatment, inappropriate targeting, and either lack of efficacy
the same regions.
or efficacy limited to only certain subgroups of patients such
Methods Three years of hip fracture data (2007–2009 inclu-
as those with demonstrable trabecular osteoporosis.
sive) were obtained from the Canadian Institute for HealthInformation for all Canadian provinces excluding Quebec.
Keywords Hip fracture . Medication . Osteoporosis .
Population information was obtained from Statistics Canada
Prescription rates
and medication information from the Brogan Inc. database.
Because osteoporosis medication is available daily, weekly,
R. G. Crilly (*)Division of Geriatric Medicine, Faculty of Medicine, The
It is an expectation of osteoporosis medications that they
University of Western Ontario, London, Ontario, Canada
reduce non-vertebral fractures as well as vertebral fractures.
The various randomized controlled trials conducted have
M. Kloseck : B. Chesworth : E. Sadowski
demonstrated that the antiresorptive agents, the mainstay of
Faculty of Health Sciences, The University of Western Ontario,
osteoporosis treatment, can produce a marked reduction in
London, Ontario, Canada
subsequent vertebral fractures and a much more modest re-duction in non-vertebral fractures From the economic
S. MequanintSchulich School of Medicine & Dentistry, The University of
perspective, reduction in hip fractures is particularly desirable
Western Ontario, London, Ontario, Canada
and has been shown in some studies but not so clearly inothers ]. In most cases, the studies were primarily designed
to reduce vertebral fractures. Patients were therefore selected
Department of Geography, The University of Western Ontario,London, Ontario, Canada
on the basis of spinal osteoporosis, as shown either by lowspine density, spinal fractures, or both. In addition to a reduc-
tion in vertebral fractures, a reduction in hip fractures was also
Division of Geriatric Medicine, Parkwood Hospital,
seen with treatment. Where selection was on the basis of hip
801 Commissioners Road East, Room A-280, London,Ontario N6C 5J1, Canada
cortical bone density, with or without vertebral fractures, a
Osteoporos Int (2014) 25:205–210
reduction in both vertebral and non-vertebral fractures was
Materials and methods
seen. However, if spinal fractures were not present, the bene-fits in terms of hip fracture reduction were more variable
This study examines osteoporosis medication prescribing
]. Generally, the benefit of treating patients with a femoral
and hip fracture rate variation by province (excluding Que-
neck T-score of better than −2.5 is minimal [].
bec and the territories) in Canada between 2007 and 2009.
Approaching the problem from the direction of the hip
fracture patient and asking how common osteoporosis actu-
ally is in these patients, it is found that although hip bonedensity predicts future fracture risk, most hip fracture pa-
The Canadian Institute for Health Information (CIHI) man-
tients do not, in fact, have particularly thin bones compared
ages health and healthcare information. CIHI's Discharge
to their peers In our series of hip fracture patients, a
Abstract Database (DAD) collects discharge statistics from
minority has a bone density that would be considered low.
Canadian healthcare institutions by procedures and diagno-
Thus, only 40 % of women and few men fall below a femoral
ses, including administrative, clinical, and demographic in-
neck T-score of −2.5 []. Similar findings have been reported
formation. The province of Quebec does not contribute to
by Stone et al. in 2003 and Siris et al. in their 2004 study
this database and so is not included in our study. Hip fracture
where only 6.4 % fell below this threshold on peripheral
data were obtained from CIHI which also provided informa-
bone density measurements. The main problem is that most
tion on physician numbers across the provinces. Brogan Inc.
fractures occur in people who are not at particularly high
collates prescription numbers from pharmacies across Can-
risk, but because of the great numbers of such people, they
ada, including prescriptions funded by private drug plans and
contribute most of the fractures. Thus, identification of these
the provincial (public) drug plans. The information available
people prior to fracture is virtually impossible and indeed the
includes a measure of the amount of medication dispensed,
benefit of treating such people is dubious. Even when they
as prescriptions as such can be written for a variable length of
have identified themselves by having one hip fracture, pre-
time. The data are collected within a forward sortation area
vention of the second hip fracture has proven difficult, pre-
(FSA), this being the geographic region used by Canada
sumably because many of the fractured patients are not from
Post. And for this study, all FSAs within each province have
the high-risk population It seems therefore that while
been amalgamated to obtain prescribing loads per province.
such treatment may benefit selected individuals with low
The FSA is the region containing the pharmacy dispensing
bone mass, the impact of this at the population level is less
the medication and not that of either the physician or the
clear and may be insufficient to make a discernable reduction
patient. The assumption is that the prescription is filled close
in hip fracture rates.
to the home of the patient, which for larger geographic areas
Studies of the changing rate of hip fracture over the past
and certainly at the provincial level, is almost certainly the
decades have shown a decline over the years and, while in
case given that healthcare and for the senior population the
recent decades there has been a rise in osteoporosis prescrip-
medication formularies are funded at a provincial level.
tion rates, a causal association cannot be presumed. Thus in
Population information was obtained from Statistics Canada
the study of change in hip fracture rate in Canada over the
2006 census data and is also available by FSA regions.
years from 1985 to 2010, while showing a steady declineover the decades and an increasing rate of decline after 1996,
it was felt that this increasing rate of decline began before theuse of bisphosphonates was sufficiently widespread to be the
All hospitalization records from 2007 to 2009, in which the
cause [Interestingly, a similar finding was seen in the
most responsible diagnosis was a hip fracture, were obtained
Netherlands with a break in the line at around 1994, while in
from the CIHI DAD and identified using the Canadian
Spain, a marked increase in prescribing produced no de-
Classification of Health Interventions [CCI] and the Inter-
crease in the hip fracture incidence [, ]. In this study,
national Classification of Diseases 10th Revision, Canada
we have explored this issue further. We have compared the
[ICD-10-CA]. Hip fractures were identified from the ICD-
use of osteoporosis medication across the provinces of Can-
10-CA using diagnosis code S72.0-.2 and from the CCI
ada, which varies widely, with the concurrent rate of hip
using diagnosis codes 1VC74LANW, 1VA53LAPMN, and
fracture to see if higher prescription rates in certain provinces
1GZ31CAND. Total annual hip fractures were calculated for
were associated with lower fracture rates. We have also done
the study period (2007–2009) and stratified by age group,
this with the intertrochanteric and subcapital fractures sepa-
sex, and province (initially 5-year intervals with aggregation:
rately to see if there is any differential effect on the two
55–59, 60–64, 65–69, 70–74, 75–79, 80–84, and ≥85 years).
fracture types, as there is evidence that the intertrochanteric
It is unclear whether readmission for hip fracture was the
fracture may be the more trabecular osteoporotic hip fracture
result of original hip fracture complications, inter-hospital
for which the antiresorptives might be more effective [
transfers, or due to a second hip fracture; therefore, all hip
Osteoporos Int (2014) 25:205–210
fracture hospitalizations were counted. Because osteoporosis
Osteoporosis Canada website for details
medication is available daily, weekly, monthly, and yearly,
), but quite different rates of
medication dispensing units were converted to days of pre-
prescribing, by a factor of almost 4. It is not explained by a
scribing, so that a once a year infusion prescription (zoledro-
difference in family physician density (or availability) as this
nic acid) represented 365 days, a prescription for a medica-
differs little across the provinces, although information about
tion taken monthly (risedronate) represented 30 days of
specialists who may have an interest in osteoporosis is not
treatment, and so forth. The number of days of prescribing
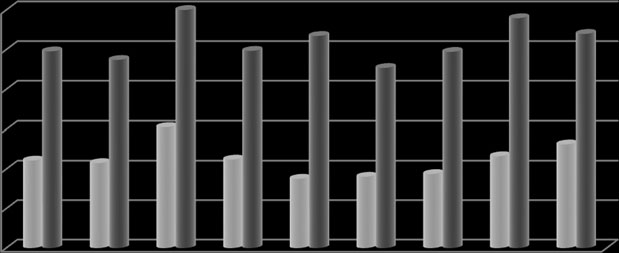
available [Figure also shows the rate of hip fracture
of the osteoporosis medications is summed to provide a
across the provinces in the same order for both men and
measure of the prescribing load for the region and time under
women. There is little difference and clearly no relationship to
consideration. The medications included in the analysis are
prescribing load.
hormone replacement therapy, risedronate, alendronate, zo-
Our prescribing data do not provide the age breakdown
ledronic acid, didronel, raloxifene, and teriparatide. For the
of the patients for whom the prescriptions are written. It is
time studied, denosumab was not yet available
possible that the impact is on the younger patients and
The denominator was generated using population data
women who may be more likely to be treated. Accord-
obtained from the 2006 census for each province excluding
ingly we have looked at the hip fracture rate across
Quebec. In addition, territories including the Northwest,
provinces for different age groups and the separate gen-
Yukon, and Nunavut were excluded from this analysis due
ders. Again, no relationship between prescribing rate and
to their relatively low population base (responsible for .25 %
hip fracture rate emerged. We repeated each of these
of the overall Canadian population).
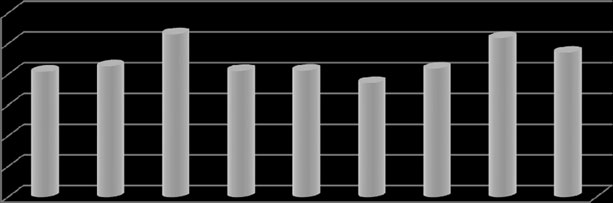
analyses for the subcapital and intertrochanteric fracturesseparately but no impact on either was apparent. As an
example, Fig. shows proportion of IT fractures in fe-males by province, and again, no effect is apparent. We
The database contained a total of 65,659 hip fracture epi-
also noted a reduction in prescribing across the 3 years of
sodes, 18,316 (28 %) in men (average age 78.48±10.90) and
the study with a decline of 15.4 % across the 3 years. This
47,343 (72 %) in women (average age 82.08±9.63). Of the
is seen in all provinces, but is not associated with any rise
total hip fractures, less than 1 % was disregarded because of
in fracture rate.
missing or incorrect postal code information.
Statistical analysis
The denominator was derived using provincial census pop-
We have been unable to demonstrate any impact of
ulation data from 2006; hip fracture occurrences and pre-
osteoporosis medication on hip fracture rate across the
scribing load were aggregated for the years 2007–2009, by
different provinces in Canada despite a wide variation
province, gender, and age group and then used to calculate
in prescribing rates. Although our data suffer from some
the annual unadjusted (crude) fracture rate. Hip fracture rates
clear deficiencies, such as lack of information about the
were standardized per 10,000 person-years and calculated
age and gender of the patients receiving the medication,
for the population over the age of 54 for each province. Rates
it is surprising that no impact is even suggested across
were adjusted to the 1991 age structure of the Canadian
age groups and either gender. Despite evidence at the
population using the direct method. Hip fracture rates were
individual level that some benefit is to be expected, we
analyzed by province for each age group and gender against
are not able to demonstrate this at the population level.
the osteoporosis medication prescribing load and number of
Prescribing does not, of course, confirm treatment and
physicians per province. The limited number of data points
the high rate of nonadherence with osteoporosis medi-
makes correlation analysis unreliable so the analysis is large-
cation is well known but is likely mostly seen in failure
ly descriptive.
to fill the prescription, so such nonadherence would notaffect our results
Targeting of patients for treatment may not be ideal, but as
the medications are likely to be prescribed for those withpoor bones shown, for example, by a low BMD, some
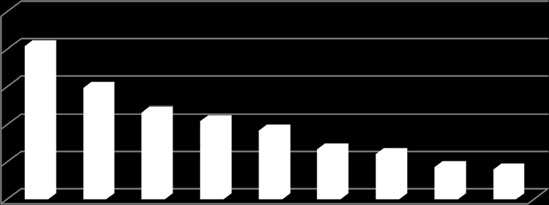
Figure shows the provinces ranked by prescribing load.
benefit in these patients may be expected. However, we
There is a substantial difference in prescribing habits across
know that most hip fractures occur in patients who do not,
the provinces. This appears to be due to a difference in practice
on BMD, have a high risk of fracture, and these may not have
habit and not accessibility to provincial formularies. For
been targeted for treatment prior to fracture. For example, in
example, Alberta and Manitoba have similar formularies (see
our own exploration of hip fracture patients in our locality,
Osteoporos Int (2014) 25:205–210
Fig. 1 The number of
osteoporosis medicationtreatment days per 10,000
population over 55 years across
the Canadian provinces for the
years 2006–2009. Sources:Brogan Inc. (medication data)
and Statistics Canada
(population data)
we found only about 30 % of women and very few men fell
population being treated and show an observed/predicted
into the CAROC high-risk zone on the basis of BMD alone
ratio of 61 %. Again, given that even for high-risk patients'
]. Thus, even with a widespread risk assessment program,
treatment is often not provided, it seems likely that this
only about 25 % of the possible fracture cases might have
would make little impact at the population level. We have
been treated, with an expected benefit of, at most, a 30 %
no information regarding the reasons for the prescribing of
reduction. Thus, a maximum benefit of a 7.5 % reduction
the osteoporosis medication. Treated patients may be a mix-
might be the most that could be expected, and, as this would
ture of those at risk because of prior fractures with others
be under ideal conditions of risk assessment, prescribing, and
deemed to be at risk for other reasons. This may all point to
compliance, the benefit may be much less. A recent report
the need for better targeting, focusing only on those with
] explored whether treatment reduces the risk of fracture
clear trabecular osteoporosis who closely resemble those in
below that predicted by the FRAX tool [This study
the original studies. Clearly, a proper ad hoc prospective
suggested an effect only in the highest risk group treated
longitudinal cohort study will be required in order to clearly
for over 5 years and who show high compliance. Although
delineate the patients appropriate for treatment with these
the authors hypothesize reasons why this does not indicate a
failure of efficacy in most treated patients, this would cer-
It may be asked if there has been time for the effect to be
tainly be one and perhaps the simplest explanation. The
seen. In most studies, a reduction in hip fracture can be
high-risk patients seem to constitute only 8.5 % of the
shown within 3 years and sometimes much sooner. The
Fig. 2 Unadjusted crude rates
by province per 10,000person-years of hip fracture by
gender (2007 to 2009)
Osteoporos Int (2014) 25:205–210
Fig. 3 Unadjusted crude
rates by province per 10,000person-years of female
intertrochanteric fracture (2007
bisphosphonates have been in the market for over 10 years
It may be that expanding the use of these medications to a
and certainly for more than 3 years prior to our study, so it
larger segment of the population may not work as their effi-
seems unlikely that this is the explanation.
cacy in low-risk individuals is open to doubt. Additionally,
We have treated all osteoporosis medications as being
although the concept of fracture risk prediction and prevention
equal. The vast majority of prescriptions are for the
is currently fashionable, most of these fractures (about 80 %
aminobisphosphonates, varying only in frequency (and
]) are non-vertebral and better predicted by cortical bone
dose) of administration. Medication may be given daily,
status. Therefore, the outcome of the current risk assessment
weekly, monthly, or yearly and use of "days of treatment"
tools [, ] is that the focus is on the type of bone least
corrects for this disparity. All the aminobisphosphonates
responsive to treatment with our current medications.
have been shown to have similar efficacy at least as far as
One remaining possibility is that there are two influences
preventing hip fractures in the mostly osteoporotic patients
at work: one being the attempt to prevent fractures by treat-
enrolled in the studies is concerned, so combining in this
ment and the other being the prescribing of medication in
manner would seem to be justified.
response to the hip fracture. Clearly, these would work in
In addition, the rate of prescribing is declining with no
opposite directions and if of equal force may cancel each
obvious effect on hip fracture rate. In this case, however, it
other out. However, evidence would suggest that the preven-
may take longer for a decline in prescribing to be reflected in
tion mode is much the greater influence and that the number
the rise in hip fracture rate.
of people started on treatment because of a hip fracture is
Lack of efficacy for the most vulnerable segment of
small. Several studies have demonstrated the low rate of
the population is another possible explanation. Most hip
osteoporosis treatment after a hip fracture , ].
fractures occur in the elderly who have fallen. Reducingfalls may reduce the fracture rate in these people, suchas has been shown in the vitamin D studies ]. We
lack evidence of efficacy of osteoporosis medication inthe elderly, the most at-risk segment of the population.
This study has shown a marked variability in the use of
We know that a fall onto the greater trochanter will
osteoporosis medications across Canadian provinces. Re-
produce sufficient force to fracture any hip and this is
gardless of the cause of this, we have been unable to show
the type of fall that characterizes the elderly person.
any impact on the rate of hip fracture in the different prov-
About 30 % of those over 65 fall each year and some
inces. Additionally, the prescribing appears to be declining
recurrently [The limited effect of medication on hip
and this is again not associated with any change in the
bone strength may be insignificant in this situation.
fracture rate across our years of study. Possible explanations
Interestingly, the one antiresorptive study to show benefit
include inappropriate targeting, insufficient penetration, or
in terms of hip fracture prevention in patients who were not
lack of efficacy of the medications to impact what appears to
particularly osteoporotic in terms of trabecular bone status
be largely a cortical bone problem.
was the denosumab study This showed a significant40 % reduction in hip fracture but also a reduced number of
Our thanks are due to Warner Chilcott Pharmaceu-
falls in the treated group which may have, at least in part, been
ticals for financial support for the study and for facilitating access to the
the mechanism of benefit.
medication data and to Brogan Inc. for the provision of the medication data.
Osteoporos Int (2014) 25:205–210
Conflicts of interest
11. Hartholt KA, Oudshoorn C, Zielinski SM, Burgers PT, Panneman
MJ, van Beeck EF, Patka P (2011) The epidemic of hip fractures: arewe on the right track? PLoS One 6(7):e22227. doi
12. Guerra-García MM, Rodríguez-Fernández JB, Puga-Sarmiento E,
Charle-Crespo MÁ, Gomes-Carvalho CS, Prejigueiro-Santás A
1. Seeman E (2012) Nonvertebral fractures: as good as it gets? Interna-
(2011) Incidence of hip fractures due to osteoporosis in relation to
tional Osteoporosis Foundation overview 12(2).
the prescription of drugs for their prevention and treatment in
Accessed 30 January 2013
Galicia, Spain. Aten Primaria 43(2):82–88. doi:
2. McClung MR, Geusens P, Miller PD, Zippel H, Bensen WG, Roux
Epub 2010 Jun 15. Spanish
C, Adami S, Fogelman I, Diamond T, Eastell R, Meunier J,
13. Nakamura N, Kyou T, Takaoka K, Ohzono K, Ono K (1992) Bone
Reginster JY (2001) Effect of risedronate on the risk of hip fracture
mineral density in the proximal femur and hip fracture type in the
in elderly women. N Engl J Med 334(5):333–340
elderly. J Bone Miner Res 7(7):755–759
3. Lyles K, Colón-Emeric CS, Magaziner JS, Adachi JD, Pieper CF,
14. Osteoporosis Canada (2012)
Mautalen C, Hyldstrup L, Recknor C, Nordsletten L, Moore KA,
Accessed 12 February 2013
Lavecchia C, Zhang J, Mesenbrink P, Hodgson PK, Abrams K,
15. Jones TM, Petrella RJ, Crilly R (2008) Determinants of persistence
Orloff JJ, Horowitz Z, Eriksen EF, Boonen S (2007) Zoledronic
with weekly bisphosphonates in patients with osteoporosis. J
acid and clinical fractures and mortality after hip fracture. N Engl J
Med 357(18):1799–1809
16. Papaioannou A, Morin S, Cheung AM, Atkinson S, Brown JP,
4. Cummings SR, Black DM, Thompson DE, Applegate WB, Barrett-
Feldman S, Hanley DA, Hodsman A, Jamal SA, Kaiser SM, Kvern
Connor E, Musliner TA, Palermo L, Prineas R, Rubin SM, Scott JC,
B, Siminoski K, Leslie WD (2010) clinical practice guidelines for
Vogt T, Wallace R, Yates AJ, LaCroix AZ (1998) Effect of alendronate
the diagnosis and management of osteoporosis in Canada: summa-
on risk of fracture in women with low bone density but without
vertebral fractures. JAMA 280(24):2077–2082
17. Leslie WD, Lix LM, Johansson H, Oden A, McCloskey E, Kanis
5. Cummings SR, Black DM, Nevitt MC, Browner W, Cauley J,
JA (2012) Does osteoporosis therapy invalidate FRAX® for frac-
Ensrud K, Genant HK, Palermo L, Scott J, Vogt TM (1993) Bone
ture prediction? J Bone Miner Res 27:1243–1251
density at various sites for prediction of hip fractures. The Study of
18. FRAX WHO Fracture Risk Assessment Tool
Osteoporotic Fractures Research Group. Lancet 342(8837):72–75
Accessed 12 February 2013
6. Cummings SR (1985) Are patients with hip fractures more osteo-
19. Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, Staehelin
porotic? Review of the evidence. Am J Med 78(3):487–494
HB, Bazemore MG, Zee RY, Wong JB (2004) Effect of vitamin D
7. Crilly RG, Cox L (2013) A comparison of bone density and bone
on falls. A meta-analysis. JAMA 291:1999–2006
morphology in those presenting with hip fractures, spinal fractures
20. O'Loughlin JL, Robitaille Y, Boivin JF, Suissa S (1993) Incidence
or a combination of the two. BMC Musculoskelet Disord 14:68.
of and risk factors for falls and injurious falls among the
community-dwelling elderly. Am J Epidemiol 137:342–352
8. Stone KL, Seeley DG, Lui LY, Cauley JA, Ensrud K, Browner WS,
21. Cummings SR, San Martin J, McClung MR, Siris E et al (2009)
Nevitt MC, Cummings SR (2003) BMC at multiple sites and risk of
Denosumab for prevention of fractures in Postmenopausal women
fracture of multiple types: long-term results from the Study of
with osteoporosis. N Engl J Med 361:756–765
Osteoporotic Fractures. J Bone Miner Res 18(11):1947–1954
22. Rabenda V, Vanoverloop J, Fabri V, Mertens R, Sumkay F,
9. Siris ES, Chen Y-T, Abbott TA, Barrett-Connor E, Miller PD,
Vannecke C, Deswaef A, Verpooten GA, Reginster JY (2008)
Wehren LE, Berger ML (2004) Bone mineral density thresholds
Low incidence of anti-osteoporosis treatment after hip fracture.
for pharmacological intervention to prevent fractures. Arch Intern
Bone Joint Surg Am 90(10):2142–2148
Med 164(1):1108–1112
23. Jennings LA, Auerbach AD, Maselli J, Pekow PS, Lindenauer
10. Leslie WD, O'Donnell S, Jean S, Legacé C, Walsh P, Bancej C,
PK, Lee SJ (2010) Missed opportunities for osteoporosis treatment
Morin S, Hanley DA, Papaioannou A (2009) Trends in hip fracture
in patients hospitalized for hip fracture. J Am Geriatr Soc
rates in Canada. JAMA 302(8):883–889
Source: http://www.theheal.ca/uploads/pdf/Comparison%20of%20hip%20fracture%20and%20osteoporosis%20medication.pdf
Increased survival of western corn rootworm on transgenic corn within three generations of on-plantgreenhouse selectionLisa N. Meihlsa, Matthew L. Higdonb, Blair D. Siegfriedc, Nicholas J. Millerd, Thomas W. Sappingtond, Mark R. Ellersiecke,Terence A. Spencerc, and Bruce E. Hibbarda,b,1 aDivision of Plant Science, 205 Curtis Hall, University of Missouri, Columbia, MO 65211; bUSDA-ARS, 205 Curtis Hall, University of Missouri, Columbia, MO65211; cUniversity of Nebraska-Lincoln, Department of Entomology, 202 Plant Industry Building, Lincoln, NE 68583; dUSDA-ARS, Genetics Laboratory, IowaState University, Ames, IA 50011; and eAgricultural Experiment Station Statistician, 307E Middlebush, University of Missouri, Columbia, MO 65211
The Sec6兾8 complex in mammalian cells: Characterization of mammalian Sec3,subunit interactions, and expressionof subunits in polarized cellsHugo T. Matern*, Charles Yeaman†, W. James Nelson†, and Richard H. Scheller*‡ *Genentech, Inc., Department of Richard Scheller, 1 DNA Way, South San Francisco, CA 94080-4990; and †Department of Molecular and Cellular Physiology,Stanford University Medical School, Stanford, CA 94305


