
Cialis ist bekannt für seine lange Wirkdauer von bis zu 36 Stunden. Dadurch unterscheidet es sich deutlich von Viagra. Viele Schweizer vergleichen daher Preise und schauen nach Angeboten unter dem Begriff cialis generika schweiz, da Generika erschwinglicher sind.
Pr1 fecal incontinence protocol
Faecal Incontinence Protocol
Printable version.
Using the NeuroTrac 5™ EMG Biofeedback for Rehabilitation of the Pelvic Floor
in Patients with Faecal Incontinence Protocol
Written By: Pirkko Raivio
Specialist Continence Physiotherapist
Dept of Physiotherapy
Central Finland Health Care District
Background information
Faecal incontinence is one of anorectal symptoms and disorders. It is a socially and
psychologically debilitating disorder that causes shame and is the most common reason to
institutionalize old people. Faecal incontinence is reported in 3%-8% of the population and in
30% in nursing home residents.
Vaginal delivery can lead to faecal incontinence due to a mechanical tear of the sphincters or a
generalized weakening of the sphincter mechanism and pelvic floor. Symptoms of faecal
incontinence are reported 13% of primiparous women,
After second vaginal delivery 20% and 7% of multiparous women ( Haadem K et al. 1997,
Kamm MA 1994, Sultan AH et al. 1997, Tetzchner T et al. 1996 ). Faecal incontinence is under
diagnosed because of not seeking healthcare and because of the attitude of doctors.
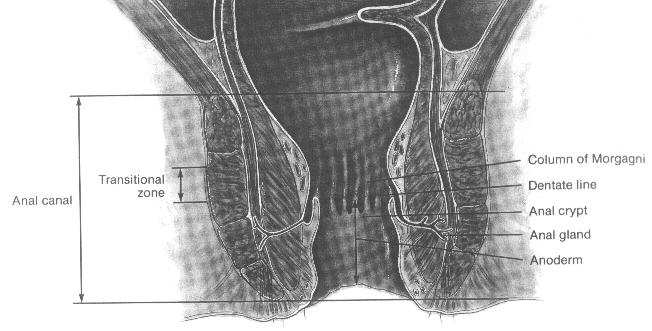
The function of the anorectum is to maintain faecal continence and to allow controlled
defecation and passage of flatus. This is achieved by the action of the anal sphincters and pelvic
floor muscles. ( Fig.1 )
The inner circular smooth muscle layer of rectum grows in thickness distally, forming the
internal anal sphincter. The internal anal sphincter is controlled by autonomous nerves and
contracted at rest. ( Höckerstedt K et al. 1998 ).
Fig.1 Lining of the anal canal ( from the book: Principles and Practice of Surgery for the Colon, Rectum, and Anus 1992 )
The external anal sphincter is striated muscle. It surrounds the internal anal sphincter and
extends 0,5-1.0 cm further down and joins the puborectal muscle without clear-cut anatomic
separation. Puborectal muscle forms a sling behind the rectum and is attached in front to pubic
bone. The activity of the external anal sphincter is continuous even during sleep. ( Höckerstedt
K et al. 1998, Marcio J et al. 1997 ).
The internal anal sphincter is supplied by both sympathetic ( L5 ) and parasympathetic ( S2-S4 )
nerves. The external anal sphincter is innervated by the perineal inferior hemorrhoidal
branches of pudendal nerves ( S2, S3, S4 ), the other parts of levator muscles receive innervation
directly from the nerve roots S2-S4. The afferent sensory fibers run directly to the plexus S4 (
Marcio J et al. 1997, Sagar PM et al. 1996 ).
Faecal continence is dependent on many different factors acting together. Factors maintaining
faecal continence are consistency of stool, delivery of colonic contents to the rectum, rectal
capacity and compliance, anorectal sensation, function of the anal sphincter mechanism and
muscles and nerves of the pelvic floor. Psycho behavioral factors have an impact on function of
the anorectum to the full defecation process. ( the American Gastroenterological Association
1999 ).
Etiological factors for faecal incontinence are
◊ altered stool consistency-diarrheal
◊ inadequate reservoir capacity or compliance (inflammatory bowel disease, absent rectal
◊ inadequate rectal sensation (neurologic conditions, overflow incontinence) ◊ abnormal sphincter mechanism or pelvic floor ( anatomic sphincter defect, pelvic floor
denervation, congenital abnormalities, miscellaneous) ( J. Marcio N. Jorge, Steven D. Wexner 1993 )
Assessment
A good history and a symptom questionnaire give information for diagnostic evaluation and
measuring of treatment efficacy in patients with faecal incontinence (the American
Gastroenterological Association 1999 )
Patient questionnaire: consistency of content lost ( gas, liquid, solid ), use of pads, limitations,
sensation at time of defecation, ability to differentiate gas/liquid/solid. Previous therapy for
incontinence, associated symptoms, past medical history, obstetric history, relation to deliverers
to dysfunction, operative history and relation of operation to dysfunction ( J. Marcio N. Jorge,
Steven D. Wexner 1993 )
Faecal incontinence grading systems ( CJ Vaizey, E Carapeti, JA Cahill, MA Kamm: Prospective
comparison of faecal incontinence grading systems, 1999 )
The Pescatori score
Incontinence for flatus/mucous
Less than once a week
At least once a week
Incontinence for liquid stool
Less yhan once a week
At least once a week
Incontinence for solid stool
Less than once a week
At least once a week
AI score = AI degree + AI frequency.
AI, anal incontinence.
The Wexner
score
Type of
Never, 0; rarely, <1/month; sometimes, <1/week, >1/month; usually, <1/day, >1/week, always. >1/day 0,perfect; 20, complete incontinence.
The newly developed incontinence score
Incontinence for solid stool
Incontinence for liquid
stool
Incontinence for gas
Alteration for lifestyle
Need to wear a pad or plug
Taking constipating
medicines
Lack of ability to defer defecation for
15 minutes Never, no episodes in the past four weeks; rarely, 1 episode in the past four weeks; sometimes, >1 episode in the past four weeks but <1 a week; weekly, 1 or more episodes a week but <1 a day; daily, 1 or more episodes a day.
Add one score from each row: minimum score = 0 = perfect continence; maximum score = 24 = totally incontinent
Diary card. Each positive answer resulted in a numerical score as listed. Maximum score per day = 10 = worst incontinence Today
Did you leak, without being
aware of it at first?
If yes, was it: gas
Did you have great urgency when you
felt you would not make it to the
toilet in time to open your bowels?
If yes, did you actually lose some stool
before getting to the toilet?
If yes, was it: pea sized
half an egg cup
Did you wear pad or use a plug of tissue paper?
If yes, did it get soiled?
Did you take Imodium (loperamide), codeine or any
other medicine today?
Clinical status (complete physical examination)
Anal endosonography
Anorectal manometry
Defecography
Electromyography
Sensory testing
balloon distension, used to detect the threshold for three common sensations, the first
detectable sensation (rectal sensory threshold), the sensation of urgency to defecate, and the
sensation of pain (often defined as maximum tolerable volume
anal canal sensation with electrical stimulation of anal canal, to quantify anal canal sensation
increasing current until sensation is reported, sensory thresholds measured in this way are
reproducible ( Ho YH, Goh HS 1995 )
Treatment
Surgical
◊ Sphincter repair in patients with a defined muscular defect
◊ drug therapy ◊ bowel habit ( diet, fluid intake, defecation posture ) ◊ biofeedback therapy combined with neuromuscular electrical stimulation ◊ home training program
Anorectal Function Re-Education, EMG Biofeedback combined with
Neuromuscular Stimulation
1.Urge incontinence
◊ without sphincter defects ◊ with awareness of the patient ◊ against her/his will because of lack of voluntary control
2. Incontinence after sphincter repair to complete functional results of surgery
The aim:
◊ to improve sensitivity to rectal distension ◊ to improve co-ordination between rectal distension and voluntary sphincter
◊ to improve muscle power, endurance and contraction speed
Biofeedback
"Biofeedback involves measuring and displaying ordinarily unfelt physiological events on
order to permit self-regulation of these events. Because Biofeedback generally presents
information concerning the mechanism of motor control, it is important to establish the proper
scope, to explore the efficacy and to examine the therapeutic mechanism(s)." ( David E. Krebs
1990 )
The electrical activity or activation of muscles can be measured on the skin surface by attaching
surface electrodes. The signals recorded in this way are called electromyograms ( EMGs ) ( Kari
L. Keskinen, Keijo Häkkinen 1990 ).
Feedback is needed for all motor learning, the trainer can become aware of success and
progress.
EMG measuring are very sensitive to different kinds of disturbances; the place and the shape of
electrode are important and the electrode must not move during the measuring. The best place
for surface electrodes is on the muscular trunk in the middle of the nervous line and the tendon.
The models of muscle activation give knowledge of the progress or going out of muscle
activation, and of reflective function during muscular action . ( Heikki Kyröläinen 1995 )
"Surface EMG appears to have a definite role in the evaluation of sphincter function and in the
use of biofeedback training" ( The American Gastroenterological Association 1999 ).
The benefits of using EMG biofeedback:
◊ Information is provided instant and directly to the patient
◊ Muscular performance is observed all the time with either auditory or visual feedback or
both and if the function of the pelvic floor is important for the patient motivation will increase with good results
◊ Threshold target levels will elicit to reach the required level and to maintain the contraction
strong enough during required time
◊ Template training using the computer screen improves co-ordination of muscles ◊ A subjective value of the quality of life is absolutely important nowadays and tells about
successful EMG training under the process
◊ Quantitative scoring of EMG activity gives objective information about the progress
throughout the therapy process
◊ Intra-anal probe to ensure perfect contact
Neuromuscular Stimulation
◊ "Neuromuscular electrical stimulation (NMES) is the application of electrical current to elicit
a muscle contraction. The use of NMES for neuromuscular rehabilitation has grown significantly in recent years." ( A.P.Bourcier & al.1999 )
◊ Always combined with EMG biofeedback ◊ "The best responses to electrical stimulation are obtained when the electrodes are placed
close to the pudendal nerves.
The position of electrodes is fundamental and the contact area must be as large as possible." (Bourcier & al. 1999) ◊ intra-anal probe to ensure perfect contact ◊ the factors to cause neural excitation and subsequent muscle contraction are resistance to
flow of current, the size and orientation of electrodes, current intensity and pulse width, current frequency, duty cycle and treatment times (J Laycock, S Plevnik 1994)
◊ NMES can "artificially" activate striated muscle by repeatedly overloading muscles and with
electrically enticed contraction targeting and training fast-twitch muscle fibres more effectively than volontial exercise
◊ increases circulation
◊ increases muscle bulk
◊ improves functional activities of pelvic floor
◊ improves sensation
◊ decreases pain
◊ decreases hypertonus of the pelvic floor.
Exercise Regime
"Functional activities rarely occur either at constant speed or constant muscle strength. All
biofeedback sessions, including procedures with active functional movement velocity, freely
change. Specific exercises help to identify the pelvic-floor muscles. The stimulation of daily
activity is a very important stage whereby a selected "home stress" or a physical task is given
initially to assess a real-life activity. It is especially helpful to have patients perform this
program while standing. Successful recuperation of daily activities is only evident if the pelvic-
floor muscle strength is coupled with the functional activity during the therapy process.
Without a program in standing position, especially with movement, neuromuscular
reeducation is pointless. To be a success, the therapy's ultimate aim is to regain perineal
blockade before stress. During the session she/he is instructed accomplish specific movements
such as coughing, rising, squatting, lifting". (Alain P. Bourcier, Jean C. Juras 1995)
The First Therapy Session:
◊ to explain pelvic floor anatomy and physiology
◊ to contract the muscles of the pelvic floor only ( isolated ) the contraction has to be light;
Strong contractions activate the deep muscles of abdominal wall ( V. Gill, P. Neumann 1999) and " The muscular and ligamentous relationships composing the lumbosacral connection are of extreme importance in stabilising the lumbar vertebrae and sacrum during the transfer of energy from the upper body to the lower extremities " ( F.H. Willard 1999 )
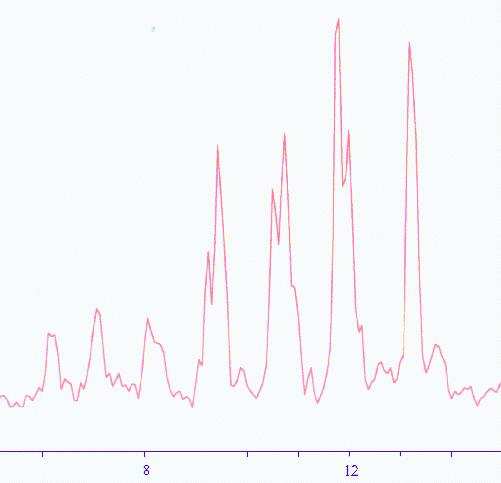
◊ quality of life score factor. ◊ investigation of pelvic floor muscle "behaviour" recording the activity during coughing
(open display); " the pubococcygeus reveals activity patterns similar to the urethral and anal sphincters at most detection sites: continuous activity at rest, some increase of activity during bladder filling, reflex increases in activity during any activation manoeuvre performed by the object (talking, deep breathing, coughing)" (D. B. Vodusek 1994)
Table 1. Coughing 7 times, position: standing
◊ Awareness of the pelvic floor musculature, to proper voluntary muscle control using
different kinds of body positions (standing, sitting, crawling, squatting)
◊ To explain the importance of the external muscle and Levator Ani in the process of
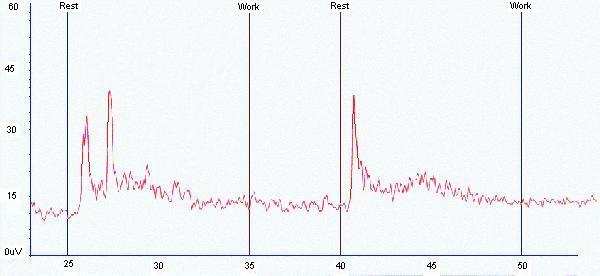
maintaining continence using the patient's own test results. (EMG Assessment 5 trials of 5 seconds work and 10 seconds rest or 5 seconds work and 5 seconds rest or 10 seconds work and 10 seconds rest), you can use so-called "evaluation test", on the ground of five, clear sub maximal repetitions; you can determine 1RM (repetition maximum), 5RM is 82% (+/- 5%). (T.Pöyhönen 1995)
Table 2, Work/Rest, position: standing
Work Statistics
Rest Statistics
Average Deviation
Average Deviation
After some minutes individual structured patient EMG template design 0,5-1minutes to see the co-ordination of pelvic-floor muscles
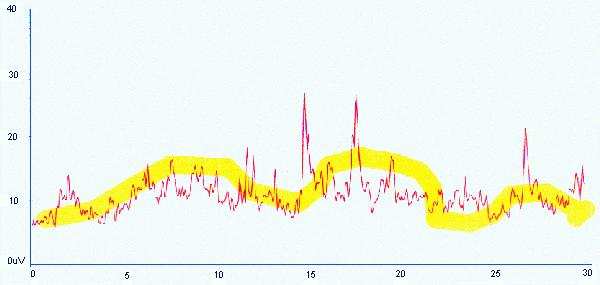
(Table 3)
Table 3, position: standing
◊ Test positions: standing, sitting or crawling, there is no sense to test in lying. ◊ "The anal canal has a greater variety of afferent nerve endings than the rectum, and they are
located in the mucosa rather than in the surrounding mesentery, the simplest technique to quantify canal sensation is to increase the current until sensation is reported. Sensory thresholds measured in this way are reproducible". (American Gastroenterological Association, AGA 1998)
The Second Therapy Session
◊ EMG Assessment 5 trials , two positions at least; standing: variety of the posture for the
contraction time; walking: double steps for the contraction time; sitting: standing up.
◊ template training on the ground of the previous results ◊ sensory training with the current ( stimulation 2-4 minutes ) ◊ EMG Controlled Stimulation ( 3-4 minutes only ) ◊ individual program for home training with ( Lock Function Mode ) or without device;
keeping a training diary if without device; 4-6 repeated contractions with adequate rest periods, at least twice the contraction time, the program 2 times a day, five days a week
◊ exercises in daily living activities
The Next Outpatient Sessions (6-7)
◊ Progressively make the sessions more difficult
◊ It is important to observe muscle fatigue
◊ Weekly or monthly measurements, new individual program and motivation to continue
◊ After these sessions it is time to evaluate, is the course right, both subjectively and
Assessment and visit to the physician after treatment; follow up at 3-6 –12 month's intervals.
References
Haadem K, Gudmundsson S: Can Women with intrapartum rupture of anal sphincter still
suffer after-effects two decades later? Acta Obstet gynscol Scand 76: 601-603, 1997
Kamm MA: Obstetric damage and faecal incontinence. The Lancet 344: 730-733, 1994
Sultan AH, Stanton SL: Occult Obstetric trauma and anal incontinence. European Journal of
Gastroenterology & Herpetology 9: 423-427, 1997
Tetzchner T, Sorensen M, Lose G, Christiansen J: Anal and urinary incontinence in women with
obstetric anal sphincter rupture. British Journal of Obstetrics and gynaecology 103: 1034-1040.
1996
Höckerstedt K, Färkkilä M, Kivilaakso E, Pikkarainen P: Gastroenterologia. Duodecim 1998
Marcio J, Jorge N, Wexner SD: Anatomy and physiology of the rectum and anus. Eur J Surg 163:
723-731, 1997
Sagar PM, Pemberton JH: Anorectal and pelvic floor function. Gastroenterology clinics of North
America 25: 163-181
Marcio J, Jorge N, Wexner Stevev D:Etiology and Management of Faecal Incontinence. Dis
Colon Rectum, January 1993 Vol. 36, No 1
Vaizey CJ, Carapeti E, Cahill JA, Kamm MA: Prospective comparison of faecal incontinence
grading systems. Gut 1999; 44:77-80 ( January )
Basmajian JV & Wolf SL: Therapeutic Exercise 1990
Häkkinen K: Voimaharjoittelun perusteet; vaikutusmenetelmät ja ohjelmointi.Gummerus
Kirjapaino Oy, Jyväskylä 1990
American Gastroenterological Association Medical Position Statement on Anorectal Testing
Techniques. Gastroenterology 1999; 116: 732-734
Apell RA, Bourcier AP, La Torre F: Pelvic Floor Dysfunction Investigations & Conservative
Treatment. Copyright 1999 by C.E.S.I
Shussler B, Laycock J, Norton P, Stanton S: Pelvic Floor Re-education Principles and Practice.
Springer Verlag 1994
Pirkko Raivio. Central Finland Health Care District, Physiatry, Keskussairaalantie 19, Fin-40620
Jyväskylä, Finland.
Source: http://veritymedical.cn/upload/documents/pr1FecalIncontinenceProtocol.pdf
PEDRO CÉSAR CANTÚ MARTÍNEZ* Medio ambiente y salud: un enfoque ecosistémico El concepto ecología, establecida en una interrelación con el resto de los seres vivos y su 1869, por Ernest Haeckel, un natu- hábitat; asimismo, con la estructura y funcionamiento ralista alemán, reconocido como pa- de los ecosistemas en general que lo acogen. De manera dre de la ecología, determina que es
Risk sharing arrangements – considerations for the future Presentation to Piperska Course Brian Godman - Mario Negri Institute for Pharmacological Research, Milan, and University of Liverpool 4. Issue and concerns Jakub Adamski – Ministry of Health, Poland 5. Group discussion 1 Risk sharing presentation 2 Risk sharing presentation The following definition is proposed based ondevelopments in Poland


