
Cialis ist bekannt für seine lange Wirkdauer von bis zu 36 Stunden. Dadurch unterscheidet es sich deutlich von Viagra. Viele Schweizer vergleichen daher Preise und schauen nach Angeboten unter dem Begriff cialis generika schweiz, da Generika erschwinglicher sind.
Code blue response-self instructional module
Implementing the ABCD's During a Code Blue Response
in an Adult Patient
Self - Instructional Module
Objectives
1. List the components of SBAR 2. Recognize the process for initiating a Rapid Response 3. Describe the process for initiating a Code Blue Response 4. Define the responders responsibilities during a code blue 5. Identify ACLS medications that may be utilized during a code blue 6. Indicate the equipment that may be utilized during a code blue 7. Explain documentation guidelines during and after a code blue 8. Describe end of code blue care 9. Discuss post resuscitation care 10. Participate in crash cart review session 11. Interpret 6 basic EKG rhythms
This self learning module is designed for the purpose of increasing nurses understanding of Code Blue Response by outlining accountabilities and practices related to staff, equipment, and processes pertaining to Code Blue issues.
Registered Nurses and Licensed Practical Nurses.
Activity
This educational activity has multiple components:
Self Instructional module with written exam
Crash Cart and monitor/defibrillator review session offered on each unit and
validated by the unit educator. Completion of this component includes: Participation in crash cart review
Demonstrate use of Likepak monitor/defibrillator
Demonstration of telemetry application EKG rhythm identification written exam and evaluation
SBAR is a situational briefing tool that logically organizes information so it can be transferred to others in an accurate and efficient manner. SBAR fosters critical thinking and eliminates information from getting lost in translation. S – Situation (why are you calling) B – Background (why is the patient in the hospital) A – Assessment (your impression of the situation) R – Recommendation (suggestions you may have)
Initiating a Rapid Response
Rapid Response is a dedicated group of individuals that responds to emergency situations within the hospital in order to try to decrease mortality and morbidity on our patients. The Rapid Responders:
Intervene in a potential code/emergency situation
Rely on bedside nurses who are highly sensitive to signs that a patient's condition is deteriorating, and empowered to call others to action.
Notification Criteria
Respiratory Rate >10 or <24
Shortness of breath Respiratory distress
Heart rate persistently > 120
Heart rate <40 Arrhythmia – Priority 1 & 2 alarms (described in Housewide Telemetry protocol)
Systolic Blood Pressure <90 mmHg
Mean Arterial Pressure (MAP) < 60 mmHg Chest Pain
Mental Status Change
Anxiety/Agitation Seizures
Urine Output <30ml/hr X 2 hours
Activation of Rapid Response
Staff indicates criteria to activate Rapid Response Staff calls "3333" (operator) and states, "Rapid Response needed in room number _"
Operator activates code pagers with message "1111 –
Patient's room number"
Assigned Rapid Responders will report to patient room
Who are the Rapid Responders?
Registered Nurse (Critical Care Services staff nurse, Clinical Nurse Manager or Charge Nurse, Nursing Supervisor) Respiratory Therapist Designated Intern
Roles and Responsibilities
Rapid Response Registered Nurse
o Arrive with tool kit o Function as a team leader in the absence of physician o Remain at bedside until patient is stabilized or transferred to appropriate
o Follow up visits 4 hours after the call for all patients not transferred to the
o Document on Rapid Response documentation form
Respiratory Therapist
o Arrive with tool kit o Function as part of the team regarding respiratory issues
Bedside Nurse
o Obtain manual vital signs o Print labs o Glucometer at bedside o Provide current situation/medical background of patient o Remain at bedside to care for patient
Unit Secretary
o Dial "3333" and state, "Rapid Response needed in room number _" o Print Rapid Response Progress note
Rapid Response in not used in Lieu of:
Code blue procedure for cardiopulmonary arrest Formal or informal critical care consult when indicated
Perform routine admission, discharge, transfer, transport functions or IV start
Exclusions to the Program
Emergency Department
ICU/CCU Operating Room
OB/Nursery with the exception of Post-Partum
Initiating a Code Blue
Code Blue refers to a patient in cardiac arrest, respiratory arrest, or any emergency situation that require resuscitation and intervention. Patient survival and positive outcomes depend on rapid assessment of the situation and initiation of basic and advanced life support measures. The first person to recognize that a patient has arrested should:
Call for help from team members
Dial 3333 and state "code blue on (nursing unit)" or delegate
someone to call a code. The code will be announced overhead and a message will be sent to all designated pagers.
Begin CPR immediately
Staff members will assist by:
Obtaining crash cart/defibrillator and immediately bring to the
patient's bedside
Place backboard under the patient as soon as possible to provide a
hard, level surface for chest compressions thus will increase cardiac output
Retrieve ambu bag, which is located in the RED box on bottom of the
crash cart and provide ventilations
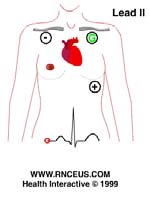
Apply electrodes and lead wires to patients chest as follows:
RA electrode (white) is applied to the right shoulder close to
the junction of the right arm and torso.
LA electrode (black) is applied to the left shoulder close to the
junction of the left arm and torso.
LL electrode (red) is applied below the heart in the abdominal
Monitor patient and EKG tracing
Placement of #18 or #20 gauge IV catheter may be necessary. If a
central line is required, the kit is located in the 3rd drawer of the crash cart. Barrier devices are located in the supply pyxis and/or drawer 3 of the crash cart: sterile towels and gloves face shields, gowns, and cap.
Responders
Director of the Code: All house staff that is near the site of the Code Blue shall respond.
Physician staff may be dismissed from the Code Blue scene after the "physician in
charge" is determined. The physician in charge must be clearly identified as being in
charge. Responsibilities include:
Direct all activities of the resuscitation effort Delegate or directly participate in airway management, vascular access,
medication orders, and maintaining Advanced Cardiac Life Support (ACLS) interventions
Recording Nurse: The nurse assigned to the patient should be the person that documents
all the events of the code for reasons of continuity in documentation and ability to
provide information regarding the patients hospitalization, current treatments,
medications and the events that occurred immediately before the code.
The recording nurse is responsible for:
Ensuring the patient chart is brought to the room when the code is called
Utilizing the Resuscitation Record to document events of the resuscitation
effort, and assists with utilization of the Crash Cart including medication and IV preparation
Place the completed Resuscitation Record in the chart. Progress notes should
indicate patient condition prior to resuscitation "code call". If necessary a "late entry" describing patient condition prior to the resuscitation event should be recorded. A notation must be made in the progress notes referring to the Resuscitation Record for events of the resuscitation
Ensuring the family and physician has been contacted
Transport patient to Critical Care Unit
Medication Nurse: This "hands on" nurse is responsible for:
Initiating BLS-HCP measures according to American Heart Association
Provide ACLS measures
Initiate cardiac monitoring
Locate/apply quick-comb redi-pak that can be utilized for defibrillation,
cardioversion, transcutaneous pacing, and viewing the cardiac rhythm.
Assess for patent IV and/or assist with the initiation of IV route
Prepare, label and administer medications per physician order
Assemble equipment for intubation and suctioning
Respiratory Therapist: Three respiratory care staff is assigned each shift to respond to
Code Blue. Respiratory Therapists responsibilities include:
Perform BLS-HCP according to AHA standards
Maintain airway by suctioning and manual ventilation before intubation
Assist physician with intubation and securing endotracheal tube (ETT) Obtaining blood sample for arterial blood gas analysis
Set up oxygen and ventilation equipment
Assist with transport to critical care unit Ensure proper paperwork is completed for the Respiratory Care Department
Anesthesiologist: If the physician is unable to intubate the patient, the operator may page
an anesthesiologist (call 3375 to confirm an anesthesiologist was contacted) to intubate
the patient, ensure an adequate airway and to facilitate ventilation.
Unit Secretary: The unit secretary must remain at the nurse's station to contact the
appropriate personnel upon request, place orders in the computer, and answer the
telephone.
Charge Nurse/Nursing Supervisor: The supervising nurse acts as a resource facilitator
for the code team. The resource facilitator is responsible for:
Communicating with personnel regarding equipment and ancillary service
Coordination of the initial resuscitation effort, assisting the recording and
medication nurse
Checking on and removing any other patients or visitors in the room as
Making space for the resuscitation effort
Clearing unnecessary staff from the room
Those who are not listed as team members and who are not actively
participating in the resuscitation effort.
Coordinating the transfer effort by contacting Registrar and/or ICU/CCU to
facilitate transfer of the patient after resuscitation.
Directing actions of the "runner".
Monitoring of the continued care of other patients Notifying the attending physician, and patient's family.
Assisting with evaluation of the resuscitation effort.
Nurse Assistant: One nurse assistant could be delegated to remain outside of the room to
assume the role of "runner". The responsibilities may include:
Running errands Obtaining supplies/equipment
Transferring patients to another area.
The remaining nurse assistants will remain on their assigned unit. When the NA is utilized as a runner, provide specific instructions regarding what is wanted, where it is located and how quickly you want it.
ACLS Medication Summary
Medications administered during a code depend on the cause of arrest, cardiac rhythm and patient's response. The goal of treatment with medications is to reestablish and maintain cardiac function, correct hypoxemia, and suppress cardiac ectopics
Most Frequently Used Code Drugs
Indication
Adult Dosage
Amiodarone
Ventricular Fibrillation (VF)
Cardiac Arrest: 300mg
Pulseless Ventricular Tachycardia (VT)
IV in 3-5 minutes (dilute
Ventricular Tachycardia (VT)
to 20-30ml D5W).
Consider repeating
150mg IV in 3-5 minutes.
Max cumulative dose:
2.2g IV/24 hours.
Wide Complex
Tachycardia (stable):
Amiodarone IVPB is obtained in Pharmacy
150mg (diluted)rapid
IV over first 10 minutes (15mg/min)
May repeat rapid
150mg dose every 10 minutes as needed
Slow infusion: 360
mg IV over 6 hours (1mg/min)
infusion: 540mg IV over 18 hours (0.5mg/min)
Atropine
Asystole or PEA: 1mg IV.
Repeat every 3-5
Pulseless electrical activity (PEA)
minutes. Max total dose: 3 doses (3mg)
Bradycardia: 0.5 mg IV
every 3-5 minutes as needed., max 0.04mg/kg
ETT: 2-3mg diluted in
10ml normal saline
Epinephrine
Ventricular Fibrillation (VF)
1mg (10ml of 1:10,000
solution) IV every 3-5
minutes. Follow each
Pulseless Electrical Activity (PEA)
dose with 20ml N.S. IV
ETT: 2-3mg diluted in
More Code Drugs
Indication
Adult Dosage
Adenosine
Narrow Complex Paroxysmal Supraventricular
With patient in reverse Trendelenburg
Tachycardia (PSVT)
position: Initial bolus of 6mg rapidly over 1-3
seconds, followed by 20ml normal saline, then elevate the extremity
Repeat dose of 12mg in 1-2 minutes
A third dose of 12mg may be given
in 1-2 minutes if needed
Known or suspected hypercalcemia;
Hyperkalemia, calcium channel
Chloride
hypocalcemia; antidote for calcium channel
blocker overdose, or IV prophylaxis
blocker or B-adrenergic blocker overdose;
before calcium channel blocker:
Prophylactically before IV calcium channel
Slow IV push of 500-1000 mg/kg
blockers to prevent hypotension
(5-10ml of a 10% solution).
Dopamine
Symptomatic Bradycardia (after atropine)
See IV Drips section below
Hypotension(SBP<70-100 mmHg)with s/s shock
Levophed
Hypotension SBP <70 with S/S shock
See IV Drips section below
Lidocaine
Ventricular Fibrillation (VF)
Cardiac Arrest from VF/VT: Initial
Pulseless electrical Activity (PEA)
dose:1-1.5mg/kg IV. For refractory
Stable Ventricular Tachycardia (VT)
VF may give additional 0.5-0.75mg/kg IV, repeat in 5-10 minutes (max dose of 3mg/kg). Single dose of 1.5mg/kg IV
ETT: 2-4mg/kg (Also see IV Drips)
Magnesium
For use in cardiac arrest only if Torsades De
Cardiac arrest for torsades de
Pointes or suspected hypomagnesemia is present
pointes or hypomagnesemia: 1-2g (2-4ml of 50% solution) diluted in 10ml of D5W IV over 5 – 20 min.
Non-cardiac arrest with Torsade de
pointes:Loading dose of 1-2g mixed in 50-100ml of D5W over 5-60 minutes. Follow with 0.5-1g/h IV (titrate to control the torsades)
Suspected ischemic pain or MI
IV infusion: 10-20mcg/min.
Increase by 5 – 10 mcg/min every 5
– 10 minutes until desired response.
Onset of actions 1-2 minutes Sublingual: 1 tablet (0.3-0.4mg) x3
at 5 minute intervals(Also see IV Drips)
Suspected ischemic chest pain
4 lpm per nc for uncomplicated MI;
100% oxygen during resuscitation
Indication
Adult Dosage
VF, Pulseless VT, may use for treatment of
Recurrent VF/VT: 20mg/min IV
PSVT uncontrolled by adenosine/vagal
infusion (max total dose: 17mg/kg).
maneuvers if BP is stable, stable wide complex
Also see IV Drips section
tachycardia of unknown origin, atrial fibrillation with rapid rate in WPW syndrome
Vasopressin
VF, pulseless VT
40 units IV single dose. May be used as an alternative pressor to epinephrine for the 1st or 2nd dose. Epinephrine may be administer 10 minutes after vasopressin
Verapamil
Alternative drug (after adenosine) to terminate
IV infusion:
Paroxysmal Supraventricular Tachycardia
Initial: 2.5-5mg IV bolus over 2
May control ventricular response in patients with Second dose: 5-10mg if needed in atrial fib, atrial flutter, and multipfocal atrial
15-30 minutes. Max dose:20 mg
ACLS Medication IV Drips
Adult Dosage
Dopamine
Mix as: 800mg dopamine in 250cc D5W
2 – 20 mcg/kg/min and titrate to
(Intropin)
Concentration: 3200mcg/ml
patients response.
Hypotension that occurs with symptomatic
Hypotension that occurs after return of
spontaneous circulation
Cardiogenic shock. May be used in
bradycardia to increase HR.
Lidocaine
Mix as: 2 grams of Lidocaine in 500 cc D5W
Maintenance infusion: 1-4mg/min
(Xylocaine)
Concentration: 4mg/ml
(20-50mcg/kg per minute)
Indications:
Significant ventricular ectopy (runs of VT, R
on T, frequent or multiform PVc's) seen in
Infusion rates:
the setting of AMI or ischemia
15cc/hr=60mg/hr=1mg/min
VT/VF that persists after defibrillation and
administration of epinephrine
VT with pulse
Wide complex tachycardia of uncertain
Mix as: 8 mg Norepinephrine in 250cc D5W
IV Infusion only: 0.5-1mcg/min
(Levophed)
Concentration: 32mcg/ml
titrated to improve BP up to
Treatment of profound hypotension
unresponsive to volume loading & dopamine

Mix as: 1 gram Procainamide in 250cc D5W
Recurrent VF/VT: 20mg/min IV
infusion (max total dose of
2 grams Procainamide in 500 cc D5W
17mg/kg).
Concentration: 4mg/ml
Administer at 20mg/min until one of
Indications: Treatment of ventricular
the following occurs:
Arrhythmia suppression Hypotension QRS widens by >50% Total dose of 17mg/kg is given Maintenance Infusion: 1-4mg/min
Renal or cardiac dysfunction: Max
total dose: 12 mg/kg.
Infusion Rates:
15cc/hr=60mg/hr=1mg/min
Tracheal Administration of Resuscitation Medications
Certain medications can be administered via the tracheal tube if unable to obtain intravenous access. Tracheal doses of medications should be 2 to 4 times higher than the intravenous route. Resuscitation medications that can be given via tracheal tube are the
"ALE" drugs.
Medication
Tracheal Administration
Atropine
2 to 3 mg diluted in 10 ml normal saline
Lidocaine
Epinephrine
2 to 2.5 mg diluted in 10ml normal saline
Recommended Technique for Tracheal Drug Administration
Prepare medication according to tracheal administration guidelines
Stop chest compressions and inject the medication via the ETT Flush the ETT with 10 ml of normal saline when indicated
Immediately attach the ventilation bag to the tracheal tube and ventilate forcefully 3
to 4 times to circulate the drug
Equipment Used in Codes
Crash Cart
All adult crash carts in the hospital contain the same basic emergency equipment and medications. To open the crash cart, turn the red plastic lock located on the bottom drawer until it breaks. Flip up the bottom panel of the crash cart and push it back firmly until it stops to be able to open the remaining drawers on the cart.
Summary of Crash Cart Contents/Location
1st drawer: 1st line drugs 2nd drawer: 2nd line drugs 3rd drawer: equipment, central line trays Bottom drawer: equipment, ambu bag & intubation box
What is not in the crash cart?
No Narcotics No Sedatives No Paralytics
Location
Quantity
Top of Cart
Monitor/Defibrillator
Quik combo redi-pak
Equipment
Suction Machine/ Canister
Clip board with Dr. Blue sheets and gray charge slips
Back of Cart
Cardiac Back Board
* Oxygen tank is located on the side of the cart
Lidocaine 2% 100mg/5ml
Atropine 1mg (0.1mg/ml)
1st line resuscitation drugs
Epinephrine 1:10,000 syringe
1mg/10ml (0.1mg/ml)
Procainamide 1 gm
Vasopressin 20 units/1 ml
Dopamine 800mg/250ml D5W
Adenosine (Adenocard) 6mg/2ml (3mg/ml)
Amiodarone 150mg/3ml (50mg/ml)
NaCl 0.9% Flush Syringes 10ml
Calcium Chloride 10% 10ml
NaCl0.9% 20 ml
Furosemide (Lasix) 40mg/4ml
2nd line emergency drugs
Norepinephrine (Levophed) 4mg/4ml (in plastic
bag with D5W 250ml to mix)
Verapamil (Calan) 5mg/2ml
Hydrocortisone (Solu-Cortef) 250mg/2ml
Romazicon 0.5mg/5ml
Narcan 0.4mg/ml
Epinephrine 1:1,000 (1mg/ml)
Benadryl 50mg/ml
Regitine 5mg
50% Dextrose 25 grams
8.4% Sodium Carbonate 50meq
Dilantin 250mg/5ml
Mag SO4 50% 2ml
Needles: 19 gauge 1 ½ inch
Syringes: 60cc
Vascular Access
Equipment; pacemaker
wire, multilumen catheter
Tapes: Non-allergenic 1 inch
Dermaclear 1 inch
IV equipment:
Tourniquets 1 inch
Scalp vein set 19 gauge
Face mask with shield
Disposable eye protector
#11 Scalpel with handle
Temporary pacing kit 5 Fr.
Pacemaker Kit includes:
Disposable pacing kit 6 Fr.
8.5 Introducer cath
EKG monitor electrodes
Vacutainer tubes (yellow, blue, gray, purple, red)
Lower shelf
Sterile gloves (6 1/2, 7, 7 1/2, 8)
IV tubing (primary, secondary, extension)
IV Fluids (0.9 N.S. 500cc & 1000cc)
IV fluids & tubing/other
Lidocaine 2 Gms.500cc D5W
equipment
Suction trays 14 Fr.
Ambu respiratory bag: RED box
Intubation tray: GRAY box
Medtronic Lifepak 20 Monitor/Defibrillator with Biphasic Technology
Delivers energy in 2 directions between the quick combo redi-pak pads
The monitor/defibrillator is located on top of the cart. The patient's cardiac rhythm can be monitored via the quick combo redi-pak or electrode and lead wires. The "lead" button or rotation of the speed dial is utilized to change the ECG lead ("Paddles refers to the quick combo redi-pak pads).
Electrical Intervention
With quick-combo
With the wire:
redi-pak:
Treat the patient not the monitor

(AED or Manual)
Immediate defibrillation is the most effective therapy for the treatment of ventricular fibrillation and pulseless ventricular tachycardia. Defibrillation delivers an electrical current to the heart to completely depolarize the heart and the impulses that are causing the dysrhythmia are disrupted. The current can be delivered through the chest wall by use of the quick combo redi-pak connected to the defibrillator/monitor for AED or manual mode defibrillation. The Medtronic lifepak in the AED mode delivers joules of 200, 300, and 360 and can only be used in cardiac arrest (unconscious patient, pulseless and not spontaneously breathing). The joules can be changed when in the manual mode. Possible complications of defibrillation include burns and damage to the heart muscle.
Anterior/Posterior
Special Considerations
ICD/Pacemaker: Avoid placing pads directly over the implanted device. Place at least
1 inch away from device.
Water: Remove patient from free-standing water and dry the chest before defibrillation.
Topical medication patches/paste (i.e. nitroglycerine): must be removed before
defibrillation.
Synchronized Cardioversion
Cardioversion is similar to defibrillation, except that the delivery of energy is synchronized to occur during ventricular depolarization (QRS complex) to disrupt the rhythm, rather than depolarize the heart. Cardioversion can be performed with a lower energy level of 50 joules. Cardioversion would be utilized in an emergency situation to treat patients with ventricular tachycardia or atrial tachycardia who have a pulse but are symptomatic (hypotension, cool clammy skin and decreased level of consciousness). Elective cardioversion can also be utilized to treat atrial fibrillation and atrial flutter.
The electrodes/lead wires and quik combo redi-pak must both be utilized for
synchronized cardioversion
Be sure to sedate the patient before cardioversion

Transcutaneous Cardiac Pacing
Transcutaneous cardiac pacing is a noninvasive
Advantages: Disadvantages:
treatment indicated for symptomatic bradycardia (HR
<60), second and third degree heart blocks. Cardiac
pacing stimulates the heart with externally applied
cutaneous pads that deliver an electrical impulse that is
conducted through the chest wall to stimulate the
myocardium. The lifepak has the transcutaneous
pacemaker option for either demand (synchronous) or
non-demand (asynchronous) pacing modes.
Demand mode: inhibits pacing when it senses the
patients own beats.
Non-demand mode: generates pacing impulses at the
selected rate regardless of the patients EKG rhythm.
The electrodes/lead wires and quick combo redi-pak
must both be utilized for pacing.
Conscious patients may require analgesia for discomfort While pacing, avoid touching the gelled area of the quick combo redi-pak or
patient to prevent electrical shock.
Do not use pads for more than eight hours of continuous pacing The patient can be paced and defibrillated through the same set of pads
Transvenous Cardiac Pacing
The patient may require transvenous cardiac
Advantages:
pacing which is a catheter that is inserted via
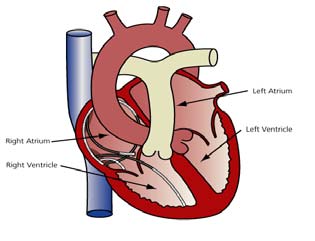
venous access. The tip of the pacing catheter The patient will Takes longer to sits against the inner wall of the right atrium,
right ventricle, or both the right atrium and
right ventricle. The proximal end of the
catheter is attached to the pulse generator.
The venous access kit and pacemaker wire
kit is located in the bottom drawer of the
External/Non-
crash cart. The pacemaker generator is
located in ICU/CCU or 2 Center. The settings on the generator are the same as transcutaneous pacing: (mA=output, rate, mode=demand or fixed).
Transvenous Pacer Supplies:
Central Line Kit: 3rd drawer
Pacer wire: 3rd drawer Pulse generator (power supply
for pacer wire): ICU/CCU or 2C
Recognition and Treatment of Dysrhythmias
Assessing the patient for hemodynamic compromising ECG changes are crucial in determining interventions and affect patient outcomes. In addition to monitoring the ECG rhythm, frequently assess the patients ABC's by:
Initiate and maintain an adequate airway to ensure adequate breathing or
Monitor blood pressure, pulse, respiratory rate, pulse oximetry (if pulse is
present) and level of consciousness
Monitor fluid and electrolytes (potassium, phosphorous, magnesium and
calcium) because electrolyte abnormalities can result in dysrhythmias
Treat the patient not the monitor
Normal Sinus Rhythm
Sinus rhythm is defined as a heart rate between 60 and 100 thus provides an adequate
cardiac output and blood pressure
Interventions:
Continue to monitor
Sinus Bradycardia
Assess for signs & symptoms of diminished perfusion with bradycardia (HR <60):
Chest pain, SOB, LOC, weakness, fatigue, dizziness, hypotension, and diaphoresis
Interventions:
Check for pulse and blood pressure If patient is symptomatic the physician should see the patient immediately.
Initiate appropriate emergency interventions.
Determine cause and treat. Causes could include: vagal stimulation,
medications causing a negative chronotropic effect, hypoxia and intracranial pressure
Consider the need for atropine (1st drawer) Consider Transcutaneous Pacing
Sinus Tachycardia
Assess for signs & symptoms of diminished p
erfusion w th tachycardia
(HR 100):
chest pain, palpitations, anxiety,
Hypotension, syncope, blurred vision,
crackles, jugular vein distention, and S3
Interventions:
Contact physician or call a code b e
Consider the need for adenosine (1 draw
Determine cause and treat There are nume
cause sinus tachycardia and all should
be considered during assessm
ent treatment and during response to treatment.
Conditions that may cause sinus tachycardia include:
Cardiac dysrhythmia
atio s/illicit drugs/poison
Respiratory distress/Hypoxia
Metabolic disorder
Head injury/ICP
Compensatory (early shock)
Emotions (anger, anxiety)
Ventricular Tachycardia
Description: Wide complex, fast and regular rhythm
Assess for signs and symptoms of diminished perfusion with VT: Hypotension,
LOC leading to unresponsiveness, and SOB. Ve
achycardia most often
precedes cardiac arrest and the patient ma
y be conscious or u
Interventions:
Assess for pulse
If the patient is stable (has a pul
ave indications of
se) and does not h
diminished perfusion: administer medications
If the patient is unstable with a pulse: cardiovert If the patient is unstable (pulseless): defibrillate
Ventricular Fibrillation
Description: Erratic electrical activity. No distinct rhythm
Signs and symptoms associated with ventricular fibrillation: The patient is in full
cardiac arrest without a blood pressure or pulse.
Interventions:
Treat for cardiac arrest
Initiate CPR according to AHA guidelines Defibrillate: 200, 300, 360 joules Consider administering
epinephrine or vasopressin (1st drawer) lidocaine or amiodarone (1st drawer)
Asystole
Description: Absence of electrical activity "flat line"
Interventions:
Check lead placement, assess for pulse Initiate CPR according to AHA guidelines Consider administering epinephrine and atropine (1st
Documentation of Code Events
A detailed chronological record of all interventions during the code must be documented on the resuscitation record. Please refer to the Policy in the hospital wide Policy & Procedure manual in the cardiology section for documentation guidelines. Documentation must include:
Time the code was called and tim
e of the physicians arriva
Staff in attendance at code interns, residents, nurses)
Time CPR was started Any actions taken Patient's response (vital signs, cardiac rhythm) Time of intubation, tube size and lip
eters (cm)
Time of defibrillation and the energy used
Time and sites of IV initiations Types and amounts of fluids administered
Time of medications given EKG rhythm strips to document events and response to treatment Disposition: Patient condition following resuscitation or transfer to ICU
End of Code
The patient should be transferred to the critical care unit as soon as possible for post resuscitation care, which includes airway management, blood pressure maintenance, oxygenation, and control of dysrhythmias. Once the patient is transferred with cardiac monitoring, ensure documentation is thorough and complete. End of code responsibilities also include:
Ensure family is contacted. If the family is present during the code, assign a
support person to inform t
of the events during and after the code
Ensure patient's physicians are contacted Clear room of equipment.
Use caution with blood and body fluids. Sharps precautions.
Take crash cart with all equipment (O2 tank, suction machine, red box, gray
box, intubation supplies and clipboard) to sterile processing with a gray charge slip indicating the patients name and medical record num
crash cart will be issued.
Support staff and have a debriefing session.
Post Resuscitation Care
In the event the patient is unable to be immediately transferred to the ICU, it is critical that the patient be monitored during the post resuscitation period. Some patients may respond after a code by becoming awake and alert while others may be unconscious. Remain with the patient while providing an ongoing physical assessment and monitoring the vital signs, pulse oximetry, and EKG rhythm. Continue to use the ABCD's (airway, breathing, circulation, defibrillation/drugs) to organize care with a goal of ensuring oxygenation and perfusion. Criteria fo
r monitoring the patient d ring the immediate post resuscitation period:
Establish a nonhostile environm
store cerebral function to optimize
oxygenation and perfusion by:
o maintaining normothermia; hypertherm
ia increases oxygen requirem
o controlling seizures; increases oxygen requirements o elevating HOB >30 degrees to increase cerebral venous drainage and
Treat hypotension per physicians orders: m y impair recovery of cerebral function
o Fluids o Inotropics
Post resuscitation VF/Pulseless VT; administer medications/treatment per
physician orders
o Beta-adrenoreceptor blocking agents o Antiarrhythmics o Magnesium sulfate o Defibrillation
Post resuscitation Tachycardia; continue to m
patient and follow
physicians orders
Post resuscitation Bradycardia; evaluate ABCD's and follow physicians orders
o Atropine o Cardiac pacing
Post resuscitation Premature Ventricular Contractions (PVC's); evaluate ABCD's
Troubleshooting the Code
Problem Intervention
Unsure "who" is in charge
State, "Will the physician in charge please
state and spell their last name"
Unsure "what" is happening
Ask clearly (i.e. please clarify drug dose)
Request that only the physician in charge
Request for anyone not directly involved in
the code to leave
Make sure one physician is in charge and
Patient not resuscitating
Think: optimal oxygenation & circulation
Pulse with compressions?
Unsure of "where" patient should go next
Ask physician if an ICU bed is needed
References
ACLS Review made Incredibly Easy (2007). Lippincott Williams & Wilkins. American Heart Association Advanced Cardiac Life Support Guidelines (2006). American Heart Association ACLS Guidelines (2003). Dulak, S. (2004). Hands-on help Temporary Pacemakers. RN Vol.67 (6) Medtronic Lifepak 20 Defibrillator/Monitor with ADAPTIV Biphasic Technology Operating Instructions Manual (2002 – 2004). Nursing 2007 Drug Handbook. Lippincott & Wilkins. Sole, Lamborn, Hartshorn, 2001. Code Management. Introduction to Critical Care Nursing, 3rd edition. W.B. Sanders
http://www.sjm.com/assessment www.brighamandwomens.org www.kidsdefib.org
Source: http://www.gch.org/documents/Nursing-Orientation/ABCDs-During-A-Code-Blue-Response-in-an-Adult-Patient.pdf
Routsias JG and Tzioufas AG. Β-λεμφοκυτταρικοί επίτοποι των ενδοκυττάριων αυτοαντιγόνων Ro/SSA και La/SSB: εργαλεία για την μελέτη της ρύθμισης της αυτοάνοισης απόκρισης. J Autoimmun. 2010, 35(3):256-64. intracellular autoantigens. Although their pathogenesis is not fully understood, autoantibodies are
Oral Tradition, 7/1 (1992):116-142 Latin Charms of Medieval England: Verbal Healing in a Christian Oral Tradition Lea Olsan This is an essay to open a discussion of medieval Latin charms as a genre rooted in oral tradition. It will concern itself solely with materials drawn from manuscripts made in England from about A.D. 1000 to near 1500. One reason for setting such limitations on the materials is that restricting the study chronologically and geographically will facilitate identification of features peculiar to the insular English tradition of Latin charms.1 For though Latin charms can be found throughout medieval Europe, to make cross-cultural comparisons prematurely might obscure distinctive regional features. To begin, it seems best to state what is meant by the word "charm" in this paper.


